A cartilage component called meniscus, aids in the appropriate function of your knee. Meniscal tears, a frequent knee ailment, are commonly treated by a meniscectomy. The purpose of the procedure is to eliminate meniscus pieces that protrude into the joint. Your knee may lock as a result of these pieces obstructing joint mobility.
Patient presented today is a 24-year-old female who complains of having pain on her left knee. The patient who had a twisting injury to the left knee while she was exercising.
Her X-ray showed no significant degenerative changes and no acute fractures. We agreed to have an MRI which showed a bucket handle tear of the lateral meniscus.
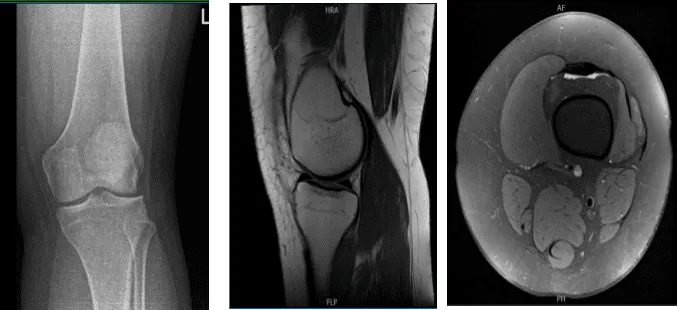
MRI of the left knee
We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, failure of surgery, need for repeat surgery, knee rehabilitation, among others.
We also discussed systemic complications including blood clots, cardiac, pulmonary, or neurological complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. Left lower extremity was put in a tourniquet. It was prepped and draped aseptically in a usual fashion. Preop antibiotic was given. Timeout was done.
A lateral entry portal was made and scope was entered. Patellofemoral compartment was normal. Medial tibiofemoral compartment and medial meniscus were also intact. The ACL was intact.
Examination of the lateral tibiofemoral compartment showed bucket handle tear of the lateral meniscus, which was rotated into the intercondylar notch. The meniscus was not able to be reduced easily and was stretched. The meniscus was released anteriorly and posteriorly at the good level. The meniscus was reduced with difficulty.
A posterolateral incision was given now behind LCL. With sharp and blunt dissection, a plane was then made between the posterior capsule and gastrocnemius.
Speculum was inserted to avoid injury to the posterior and medial aspects of the neurovascular bundles. Repair of the lateral meniscus was done with the use of inside out sutures using zone specific cannulas x3, use of Final pictures were taken and saved.
The knee was thoroughly irrigated and drained. Closure was done in layers using #2-0 Vicryl, and # 3-0 Monocryl, and # 3-0 nylon. The 0.25% Marcalne was instilled into the joint.
Dressing was done with use of Xeroform, 4×8, ABD, Webril and Ace wrap. Knee immobilizer was applied and the patient was extubated to recover in stable condition.
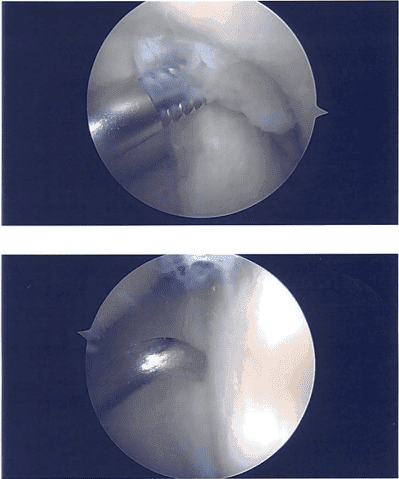
Intraoperative images
The patient underwent postoperative evaluation and was determined to move through with formal physical therapy as well as a home exercise program for knee rehabilitation. We’ll keep applying ice and elevating the knee to relieve pain and swelling while also lowering the risk of a deep vein thrombosis.
We’ll also use early mobilization and mechanical prophylaxis. As long as there are no contraindications to these meds, we will advance to anti-inflammatories and Tylenol after we have weaned them off of any narcotic medications. She will also continue taking aspirin. In three weeks, I’ll meet them again to assess their development.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
