A lateral meniscus tear affects the semicircular cartilage that lines the exterior of the knee joint. Through twisting or a traumatic injury, trimming the cartilage shock absorber is known as partial meniscectomy. Chondroplasty, or bone-coating articular cartilage trimming.
A 57 year-old female driver visits the office with left knee pain. She works as a School bus driver and she smokes. She went to Brookhaven hospital where X-rays were done and she was sent with medications. She is limping. The patient was seen in the office a couple times as part of the preparation of the surgery.
MRIs were reviewed and discussed by the doctor; There is no acute fracture or osteonecrosis. Moderate medial collateral ligament sprain/partial tear is likely reactive. The cruciate and collateral ligaments are otherwise within normal limits.
The lateral meniscus is intact. Focal full-thickness cartilage fissuring is identified in the posterior lateral tibial plateau with mild subchondral edema. There is increased intrasubstance signal abnormality within the body and posterior horn of the medial meniscus with an incomplete radial tear at the body-posterior horn junction.
No displaced fragment is seen. The posterior root attachment is intact. There is moderate thinning of the central weight bearing cartilage. Patellofemoral compartment: There is patella alta and lateral patellar tilt. Softening of the patellar cartilage is noted without full-thickness defect.
Faint edema within the lateral head gastrocnemius muscle may reflect mild strain. No high-grade disproportionate muscle atrophy is seen. The imaged tendons, inclusive of the extensor mechanism, are intact. There is a small joint effusion. No popliteal cyst is appreciated.
There are no intra-articular ossific loose bodies. Subcutaneous edema is nonspecific, the neurovascular structures demonstrate normal course. Medial meniscus tear and medial collateral ligament sprain/tear. Elsewhere most pronounced in the medial compartment. Small joint effusion.
We discussed treatment options. The patient opted for surgical management in the form of arthroscopic surgery.
We discussed the risks and complications including infection, bleeding, injury to small nerves and vessels, need for rehabilitation, development of arthritis and possible need for knee replacement in the future, system complications including blood clot, cardiac or pulmonary complications, neurovascular complications including death.
The patient consented and signed informed consent.
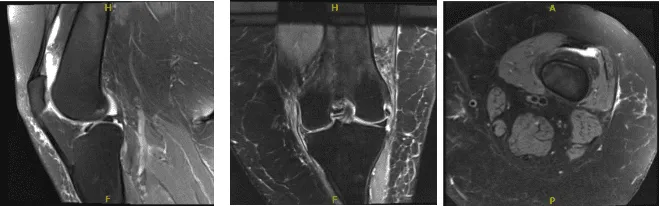
MRI Left Knee non-contrast
The patient was taken to the operating room where she was placed on a well-padded operating room table. General anesthesia was induced. Sedation was given to the patient.
Intraarticular injection of 15 cc of 2% Lidocaine and 15 cc of 1% Marcaine mixed with epinephrine was injected into the knee to achieve a local block. Tourniquet was applied. Preoperative antibiotics were given. A time was called. The left leg was prepped and draped subcuticularly in the usual fashion.
A lateral anterior portal was made and the arthroscope was inserted. A medial anterior portal was made using a spinal needle. Examination of the medial tibial compartment showed a radius tear of the posterior body of the posterior horn of the medial meniscus.
Resection of the margins of the tear was performed with the use of biters and shavers which achieved balanced margins. There was a horizontal tear also which was debrided. Balanced margins would be achieved. There was Grade III to Grade IV osteoarthritis of the medial femoral condyle.
Examination of the infrapatellar notch showed an intact ACL. Examination of the lateral femoral compartment showed intact meniscus and cartilage of the lateral tibiofemoral compartment.
Examination of the patellofemoral compartment showed Grade I to Grade II tear of the cartilage of the patella which was debrided with the use of a shaver. The knee was thoroughly Irrigated. Final pictures were taken and saved.
Closure was done with the use of 3-0 nylon. Dressing was done with the use of Xeroform 4 x 8, ABD, Webril and ACE wrap. The patient awakened and moved to the recovery room in stable condition.
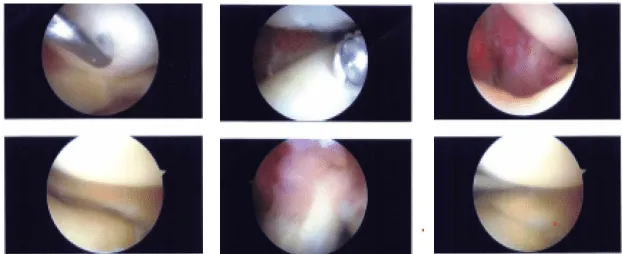
Intraoperative Images
The patient is here today status post left knee medial meniscectomy and chondroplasty. After the doctor discussed treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee.
We removed the stitches during the visit. We will continue with ice and elevation of the knee to decrease swelling and pain. We will continue to utilize early mobilization and mechanical prophylaxis to reduce the chances of a deep vein thrombosis.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications. The patient will be back in three weeks’ time to evaluate their progress.
After the surgery she continued taking physical therapy. With regular visits in the office, the patient did well and continued physical therapy for the knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
