The patient is a young 24-year-old female who presented to our office after sustaining any injury to the right wrist. The patient sustained an injury to the right wrist after falling from her bike. She had her wrist splinted at the local urgent care. She complained of swelling, pain, and loss of function at the right wrist. The pain was rated as severe in intensity and sharp in character and was aggravated with any movement of the right wrist.
The patient’s medical history was remarkable for polycystic ovarian disease and she was currently on metformin and oral contraceptive medications. The patient denied any past surgical history. She is a nonsmoker and denies the use of any illicit drugs. She has no known drug allergies.

X-ray of the wrist in oblique view showing a comminuted fracture of the distal radius.
On physical examination, there was swelling and tenderness at the right wrist. The distal neurovascular examination of the right hand was normal. X-ray and CT scan of the right wrist revealed a comminuted fracture of the right distal radius, fracture of the ulnar styloid, and disruption of the distal radio-ulnar joint (DRUJ). She had a prior closed reduction at the urgent care which was not adequate.
Various treatment options were discussed at length with the patient and she opted for surgical management. The risks of infection, bleeding, injury to adjacent nerves and vessels, and systemic complications among others were discussed at length with the patient. The patient understood and signed the informed consent.
PREOPERATIVE DIAGNOSES:
- Comminuted fracture of the distal end of radius, right wrist.
- Fracture of the ulnar styloid, right wrist.
- Dissociation of radioulnar joint.
POSTOPERATIVE DIAGNOSES:
- Comminuted fracture of the distal end of radius, right wrist.
- Fracture of the ulnar styloid, right wrist.
- Dissociation of radioulnar joint.
OPERATIONS:
- Open reduction and internal fixation of the distal radius using Stryker plate and screws.
- Transfixation of the radioulnar joint using two K-wires.
DESCRIPTION OF THE PROCEDURE: The patient was taken to the operating room where general anesthesia was induced. The right upper extremity was prepped and draped aseptically in the usual fashion. Tourniquet was applied. Preoperative antibiotics were given. Time-out was called. Tourniquet was elevated to 250 mmHg. Tourniquet time was 61 minutes.
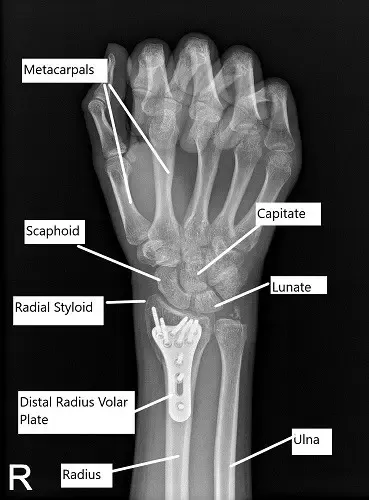
Post-operative x-ray of the right wrist in PA view.
Provisional fixation of the fracture was done after reduction using K wires. A volar incision was driven along the tendon of the flexor carpi radialis. The anterior sheath of the flexor carpi radialis was opened. The tendon was retracted medially. The posterior sheath for the tendon was opened and the pronator quadratus was reached. The pronator quadratus was incised along the radial border.
The fracture was opened. The fracture was thoroughly washed. Reduction of the fracture was again done and the wires were re-inserted. A short plate was applied under the volar aspect of the radius and fixed with olive wires. X-rays were done to check satisfactory position. The fixation of the plate to the proximal fragment was done by a single unicortical
screw.
Finding the fracture and the plate in an acceptable position, the distal fragment was fixed using locking screws including two radial styloid screws. The first screw was a cortical screw to pull the plate to the bone. The cortical screw was wasted at the end of the procedure. The proximal fragment was fixed using a combination of locking and non-locking screws. The final fixation of the plate was checked in AP and lateral views and found to be satisfactory.
Transfixation of the radioulnar joint was performed using K-wires. The final pictures were taken in AP and lateral views and saved. The wound was thoroughly washed and closed in layers using #2-0 Vicryl and #4-0 Monocryl. Dermabond was used for the skin. The dressing was performed using 4 x 4s, Xeroform, Webril, posterior long arm splint, and Ace wrap. The patient was moved to Recovery in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
