Human knee has part called anterior cruciate ligaments or ACL located in the center of our knee that helps us to prevent tibia from moving forward to the femur. The ACL is prone to tear for it looks like a string attached between tibia and femur.
Most people who experience a tear ACL feel pain and hear popping sounds whenever they try to move their knees. Torn ACL is curable by doing arthroscopy but it requires immediate care because our knee is a complex structure that needs to work together.
Patient is here with complaints of left knee pain. He is 26 year-old and currently employed as an electrician. He hurt his knee three months ago and is unsure exactly how, maybe he twisted it accidentally. He is not able to bend or extend the knee and is hopping with a limp and not able to bear weight on the foot. He is here with X-rays on his left knee.
X-ray results showed that there is mild lateral compartment joint space narrowing. We discussed treatment options on his condition including Physical Therapy, MRI, Injection and Surgery. We agreed to go with 3 tesla MRI left knee, he also agreed to start the PT and continue Rest/Ice/Compression/ Elevation Therapy.

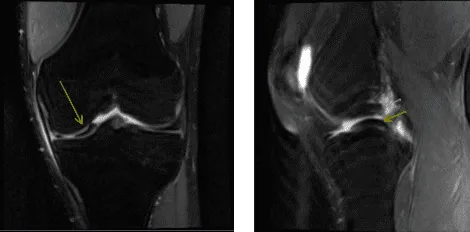
MRI of left knee
After a week the patient returned for follow-up with an MRI result. It showed an impression of abnormal morphology of the ACL likely related to partial disruption or possibly complete disruption and Medial meniscus bucket-handle tear.
MRI of left knee
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, need for rehabilitation, possibility of failure, need for repeat surgery, development of knee arthritis and possible need for knee replacement in the future, among others.
We also discussed systemic complications including blood clot, cardiac, neurologic, or pulmonary complications among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. His left lower extremity was prepped and draped aseptically in the usual fashion after application of tourniquet. Preop antibiotic was given. Time-out was called.
Examination under anesthesia was performed which showed ACL laxity or Lachman test with no end point. A lateral entry portal was made. Arthroscope was entered and a medial entry portal was made with the help of spinal needle.
Examination of the knee showed a bucket handle medial meniscus tear right from the posterior horn to the mid body. It also showed avulsion and injury to the ACL with collapse. The lateral compartment showed no tear or injury. Patellofemoral compartment was normal. We decided to harvest the quadriceps autograft as was planned.
The arthroscope was removed and a 3-cm incision was given over the proximal pole of the patella. The subcutaneous tissue and paratenon were cut in the line of excision. RayTec was used to delineate the tendon. Arthrex preset quadriceps harvest double knife was used and the tendon was cut on either side.
The distal end was elevated from the proximal pole of the patella using a blade. Proximally, the tendon was cut through the intrasubstance. Tendon cutter was used to harvest 18 mm of tendon. FiberTape was applied over the proximal femoral side.
Tendon was prepared on the back table and the tibial side was also prepared. In the meantime, an arthroscope was inserted into the knee again. Inside out repair of the medial meniscus was planned using zone-specific cannulas from the meniscus were used. Sequential from the posterior horn to the mid body.
All the needles were retrieved out of the medial knee. The needles were cut and the sutures were held by a hemostat. ACL debridement was performed. The femoral attachment of the ACL was prepared using the shaver. Tibial attachment was also prepped using the shaver.
ACL femoral jig was used and inserted. Incision was given over the lateral femoral condyle and the fascia was cut in the line of Incision. The Jig was introduced into the knee and connected The jig was passed onto the bone and punched inside.
FlipCutter was used and drilled into the knee. Once the drill was inside the knee, it was flipped back and a 25-mm turnover was made. The reamer was again inserted back into the knee and flipped back to the normal position and retrieved out. A FiberLink was inserted and retrieved.
Similarly, a tibial tunnel was made using a tibial jig for the medial portal. A 60-degree angle was used. FlipCutter was used again to make a 30-mm tunnel in a similar fashion. A FiberLink was inserted and the suture was held on to each other.
Once the quadriceps tendon was ready, it was marked and inserted over the FiberLink on the femoral side and passed into the tunnel. Then, the tibial side was also passed to the tibial tunnel using the FiberLink.
Once the tendon was in place, it was tightened on either side and found to be in a good position. The graft was tightened over the tibial side and was tightened over the button along with two 4.7 size SwiveLock. The knee was cycled 30 times before final tightening. The knee was thoroughly irrigated.
The final pictures were taken and saved. The tendon was found to be in good tension. Notchplasty of the lateral femoral condyle was performed also. The final pictures were taken and saved. Tourniquet was released at this time.
Now, posteromedial incision was given along the posterior margin of the MCL. Blunt dissection of the subcutaneous tissue and fascia was done. All the sutures were retrieved along the posterior margin of the capsule and the lateral margin of the capsule. All the sutures were tied on each other and cut.
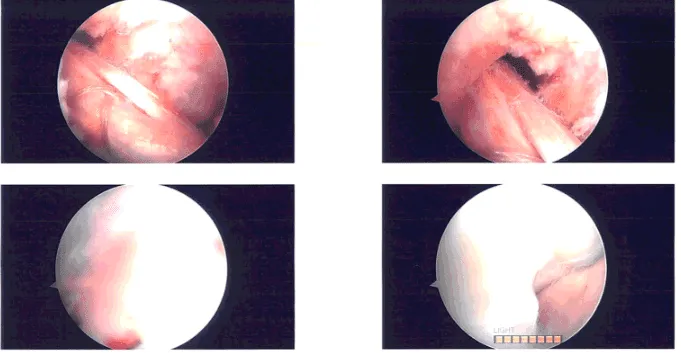
Intraoperative Arthroscopy Images
The incision was thoroughly irrigated and closed in layers using # 2-0 Vicryl and Monocryl. The quadriceps harvest incision was also closed with # 2-0 Vicryl and Monocryl. The arthroscopic portal as well as tibial and femoral ACL groove tunnel were closed using #3-0 nylon.
Dressing was done using 4 x 4, ABD, Webril, and Ace wrap. A knee immobilizer was applied after the surgery. The patient was extubated and moved to recovery in a stable condition.
After discussing the options for treatment and the risks of aspiration and injection, the patient wished to proceed with the aspiration and injection to reduce pain and swelling. After a sterile prep, and the injection of a local anesthetic, 90 cc of straw-colored fluid was aspirated from the left knee joint.
This was followed by an intra-articular injection, consisting of 60 mg or Toradol followed by 1 cc of 1% lidocaine, 1cc of 0.5% Marcaine. The patient tolerated the procedure well and there were no complications.
Post aspiration pain, and the signs of infection were discussed in detail. Patient checked in for follow up visit after a month and seen significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
