We can tell that there is something wrong in our shoulder when we feel pain, or having difficulties to move our shoulder normally. Shoulders have a big impact on our daily lives because we used to lift, push, and pull every day.
Aside from the outer pain, our shoulder has the impression of being out of its socket that needs immediate care from an Orthopedic.
In a serious injury that requires surgery, one of the most popular surgeries is called Debridement where the Surgeon expands the joint to have more space to examine the damage. It helps surgeons to see if there is tear on articular side, Glenoid Labrum or in any part of the shoulder.
Patient is a 61 year-old male and has complaints about his right shoulder and neck pain from a motor vehicle accident that happened five months ago. Per X-ray that he presented we suspected that he has right shoulder partial tear of infraspinatus with AC joint widening.
His MRI showed an impression as follows: Focal grade 1 partial-thickness tear of the infraspinatus tendon at the footprint with adjacent small traction cysts. Intact labrum and biceps tendon. Widening of the AC joint suggestive of chronic AC joint separation versus a previous. Mumford procedure. Correlate with surgical history.
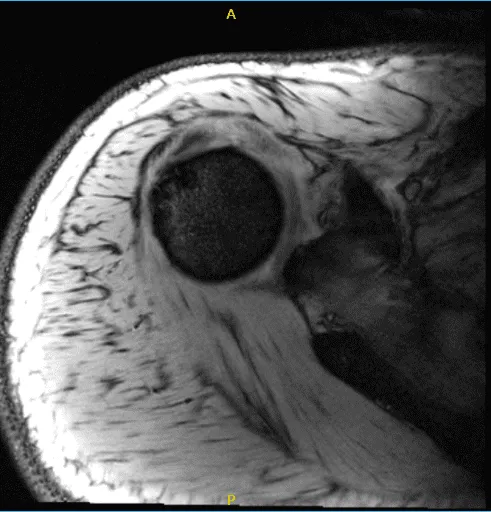
MRI of the right shoulder
We discussed treatment options and opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, rehabilitation, failure and need for repeat surgery, and systemic complications among others. The patient understood and signed the informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. Preoperative antibiotic was given. The patient was turned into the left lateral position and head in the position of a bean bag. All the bony prominences were well padded.
Axillary roll was inserted. The right upper extremity was prepped and draped aseptically in usual fashion. Time-out was called. Posterior and anterior portal was made to incision over the soft point of the glenohumeral joint.
Arthroscope was entered and examination of the glenohumeral joint showed degeneration of the glenoid labrum with tear of the superior labrum and biceps anchor. There was tearing of the subscapularis muscle as well as supraspinatus on the articular side.
Shaver was used for debridement of the rotator cuff. Straight biter was used to cut the biceps and glenoid labrum was debrided using a shaver. Rest of the examination of the shoulder joint was normal. All the pictures were saved.
The arthroscope was entered into the subacromial space, where subacromial bursitis was present. The subacromial bursitis was debrided using a shaver through an anteromedial portal. A lateral portal was made. The scope was entered through the lateral portal and further debridement was done.
Acromioplasty was performed using a thermal wand followed by a shaver. AC arthritis was seen. Distal clavicular excision was performed using the thermal wand and burr. Rotator cuff was examined and found to be intact on the bursal side. Pictures were taken and saved.
The shoulder was irrigated and drained. Now, the traction was removed and the arm was put in abduction and external rotation. Incision was given for subpectoral tenodesis along the anterior border of the pectoralis major.
The fascia was cut in the line of incision. A subpectoral approach was made to the proximal humerus. The short head of the biceps was found and delivered.
Whipstitching was done using FiberLoop. Part of bone along the bicipital groove was cleaned using the Bovie and periosteum. Beath pin was used to drill bicortically followed by unicortical drilling for the button. The tendon was noted on the button and inserted bicortically and flipped.
The sutures were tightened End of the suture was passed through the tendon and knotted The sutures were tightened. End of the suture was passed through the tendon and knotted to itself. The button was inserted over the tendon after passing one end of the suture through it.
After the button was tightened, the suture was again tied over each other. The wound was thoroughly washed and drained. Picture was taken and saved. Closure was done in layers using #0 Vicryl, 2-0 Vicryl, and 4-0 Monocryl.
The arthroscopic ports were closed using 3-0 nylon. Dressing was done using Xeroform, 4 x 4, ABD, and tape. Shoulder immobilizer was applied. The patient was extubated and moved to recovery in stable condition.
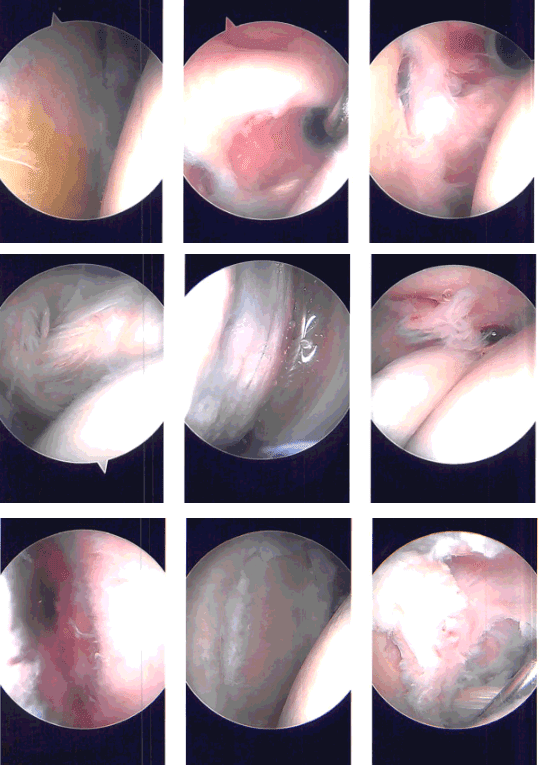
Intraoperative Arthroscopy Images
Patient returned to the office after a week post-operative. He denies chills and fever. Post Operative Exam: General Appearance: no swelling, tenderness, or warmth and wound clean and dry, appropriate range of motion, and neurovascular intact.
After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. We removed the stitches during today’s visit. We will continue with ice and elevation of the shoulder to decrease swelling and pain.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications at today’s visit
Asked the patient to return after 8 weeks post-operative and clearly showed that he got well from surgery. He said he feels relieved with the continuous physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 22, 2025.
