Case Study: Rotator Cuff Repair, Debridement, Subacromial
Decompression and Acromioplasty of the Left Shoulder in a
53-year-old male involved in an automobile accident
A 53 year-old male patient has arrived at our office complaining of lower back, left knee, and left arm pain. The pain began around a week ago. The patient recalls being injured in an automobile accident. The pain is only moderate in intensity.
The pain is continuous and interferes with sleep. The pain is accompanied with numbness. There is no swelling, bruising, tingling, radiating pain, weakness, bowel or bladder anomaly, gait trouble, giving way, or limping, or difficulty with hand function.
Since its inception, the issue has gotten worse. Walking, bending, and, finally, stairs aggravate the discomfort. Rest alleviates the symptoms. The patient had surgery on his left knee 5 years ago.
Upon examination of the left shoulder, the patient sits with the scapula protracted and depressed. They are tender to palpation over the anterior supraspinatus and proximal biceps. There is mild palpable crepitus in the subacromial space with ranging.
The patient has restricted range of motion at the last 20 degrees of overhead abduction, and discomfort with above shoulder range of motion. The patient has discomfort with impingement maneuvers Whipple testing. The shoulder is stable on exam. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth or skin lesions present.
Xray were presented and discussed. His left humerus showed unremarkable radiographs and there is angulation in the middle one third left of his clavicle consistent with prior trauma. Patient agreed to start the conservative treatment as physical therapy.
After a week, the patient returned because his left shoulder is bothering him again. The pain is worsened with activity. He got cortisone which helped. He is not able to lift the arm and carry weight. His motion is restricted and feel weak. Advised patient to undergo MRI.
Result showed that there is a grade 3 partial-thickness interstitial tear at the supraspinatus tendon insertion comprising approximately 50 percent total tendon thickness.
There is a bursal surface component to the tear at the anterior leading-edge insertion of the supraspinatus tendon and accompanying subacromial subdeltoid bursitis. Cystic changes are noted for greater tuberosity adjacent to the tear.
Though cortisone helps the patient’s condition, we decided to proceed with surgical treatment. We discussed treatment options and the patient opted for surgical management.
We discussed risks and benefits Including bleeding, Infection, failure, need for repeat surgery, need for rehabilitation among others. We also discussed injury to adjacent nerves and muscles. The patient understood and signed an Informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. He was turned into a right-sided position with the left shoulder up.
The left shoulder was prepped and draped aseptically in the usual fashion. The left shoulder was put in 50 degrees of abduction and 10 degrees of flexion. Time-out was called. Preoperative antibiotic was given.
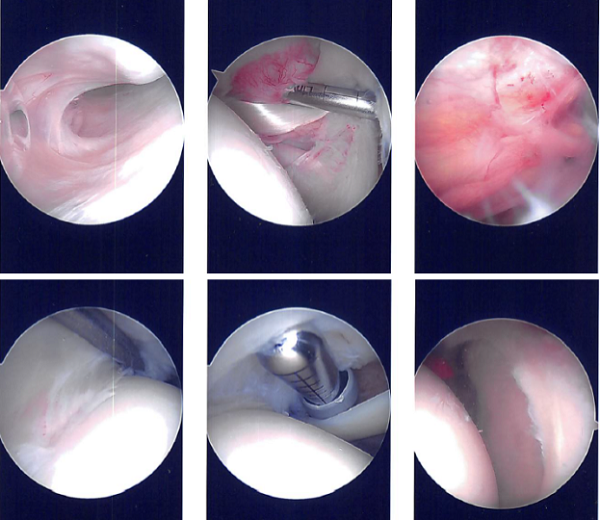
Entry portal was made through the posterior soft spot through the glenohumeral joint. Anterior entry portal was then made using a spinal needle. There was fraying of the superior labrum. It was cleaned with a shaver. There was tearing of the anterior margin of the supraspinatus.
There was a sub labral hole which was left as it is. There was minimal chondral damage to the humeral head. After shaving off the fraying of the anterior edge of the suprascapular tendon, the scope was entered into the subacromial space. Subacromial bursitis was present which was debrided using a shaver.
There was acromial spurring which was cleaned using a bur and sub acromioplasty was performed. After a thorough sub acromioplasty and release of CA ligament, the rotator cuff was inspected.
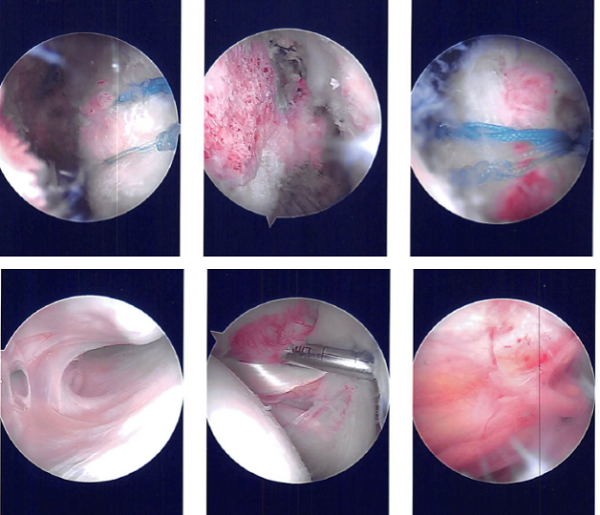
It was found to have a partial tearing into the anterior margin of the supraspinatus. It was a high-grade partial tear which was completed by use of the shaver. The tear was cleaned. The bony footprint was cleaned using a shaver and bur.
Entry was made using an awl for the two-tailed Healicoil biocomposite suture from Smith & Nephew. The anchor was inserted. A separate entry portal was made for bites of the rotator cuff tendon.
First pass was used. Sequential bites were taken at both sites through the rotator cuff tendon and checking that the biceps was spared. Sutures were tied on to each other for the medial row. A lateral row was planned using a Bio-Anchor. All sutures were passed through the anchor and Inserted Into the humeral head.
Final pictures were taken and found to be satisfactory. The pictures were saved. The distal clavicle was showing operating changes and distal clavicle excision was not performed. The shoulder was thoroughly washed and drained.
Closure was performed using #3-0 nylon. Local was injected. Dressing was performed using Xeroform, 4 x 4, ABO, and tape. An Abduction shoulder immobilizer was applied.
After a week post-operative, the patient consulted again in our office. He is doing fine and his pain has improved. He is using a shoulder immobilizer. Examination of the left shoulder reveals that the incisions are healing well, without evidence of drainage, erythema or warmth.
Range of motion and strength are progressing appropriately at this stage of rehabilitation. Strength remains 5/5 distally. There is no tenderness at the elbow and wrist. Sensation is intact to light touch distally and there is a brisk capillary refill.
We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.

Dr. Vedant Vaksha
I am Vedant Vaksha, Fellowship trained Spine, Sports and Arthroscopic Surgeon at Complete Orthopedics. I take care of patients with ailments of the neck, back, shoulder, knee, elbow and ankle. I personally approve this content and have written most of it myself.
Please take a look at my profile page and don't hesitate to come in and talk.