A twisted knee is a common issue that can damage the knee’s ligaments and cartilage. It frequently causes discomfort and swelling, as well as instability and functional limitations.
Self-care measures are effective for many kinds of minor knee pain. Physical treatment and knee braces can also help alleviate pain. However, in some instances, your knee may require surgical repair.
Patient was presented in the office with a complaint of having knee pain because of an injury that caused his knee to twist. The pain is mild in intensity. It is associated with swelling. Patient describes the pain as aching. The pain is coming and going by bus does not disturb my sleep.
The problem has been getting better since it started. Walking and standing aggravated the pain. Rest down makes the symptoms better. The patient has undergone surgery for the same in the form of ACL reconstruction and bucket handle meniscus tear repair three years ago.
Upon examination of the right knee, the patient is tender to palpation along the medial joint line, and has an effusion. Healed scars from ACL reconstruction with Hamstrings autograft. The patient has discomfort with McMurray’s maneuvers, and the knee is stable. ACL intact on Lachman test.
They lack full extension, but have full flexion. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth or skin lesions present.
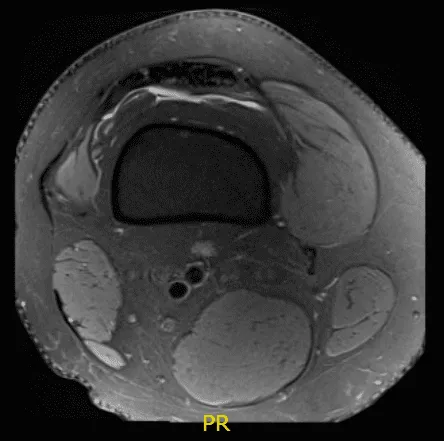
MRI result received, there is status post anterior cruciate ligament reconstruction. The graft is intact. Tubular cyst formation is present within the tibial tunnel. There is a large bucket-handle tear of medial meniscus, displaced into the intercondylar notch and over anterior horn.
There is a tiny capsule remnant posteriorly and peripherally. The lateral meniscus demonstrates free margin fraying of posterior horn and adjacent body aspect without substance tear.

Arthroscopic surgery was performed. Lateral anterior portal was made for arthroscopic viewing. The scope was entered and the camera was entered. The camera showed a tear of the posterior horn and brought the posterior body of the lateral meniscus around the popliteal hiatus at its periphery.
The tear was repairable and I decided to repair it. There was a grade 2 to grade 3 chondral lesion over the patella as well as lateral condyle of the femur. Chondroplasty was performed. The meniscal rasp was used to prepare the capsular as well as the meniscal attachment.
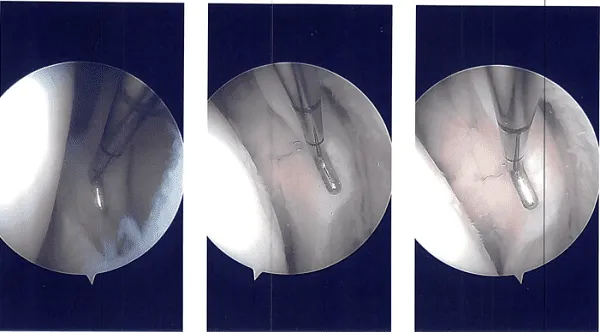
A plane was made between the popliteus and the gastrocnemius with the vessels behind. Sims speculum was used to retract the vessels posteriorly. Another scope was reintroduced on the lateral border and all-inside repair was done using FasT-Fix with a Nephew curved all-inside implant and sutures.
Three of them were put in the body posterior and medial to the popliteus muscle and one was put lateral to the popliteus muscle. The reduction and repair were found to be adequate. The tourniquet was released and found to have a good blood clot inside.
The Incision was closed. Marcaine 1% 10-cc were put into the joint. Dressing was performed using 4x4s ABD, Webril and Ace wrap. Bledsoe knee brace was put with locked in extension. The patient was moved to the postoperative care unit after extubation in a stable condition.
After a week of postoperative surgery, he had been using a knee brace (ROM) and denied fever and chills. A month after, the incisions were healed well, without evidence of drainage, erythema or warmth. He was advised to do physical therapy and take some anti-inflammatory drugs until he had full relief.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.