We humans intend to lift heavy things, especially in our daily lives. While we are at the gym, school, in our house doing chores, and of course if we are skilled labor workers. Stronger upper body muscles aid in the lifting of large goods in regular duties.
Our rotator cuff muscles work together to stabilize the shoulder joint by producing movements of the humeral head inside the glenoid fossa.
Patient is here today with complaints of left shoulder pain. He is unsure of how he got the injury. The patient works full time as a foreman, and helps his colleague to lift heavy materials most of the time.
He is here with an X-ray of the left shoulder. He is left hand dominant. He is not able to work due to pain. He has tried stretching at home, and Tylenol to no benefit.
His X-ray showed normal left shoulder radiographs so we decided to get an MRI to see the reason for the pain.

MRI of left shoulder
His MRI showed a complete tear of the supraspinatus tendon with 8 mm of medial retraction. Mild infraspinatus and long head biceps tendinosis and mild subacromial/subdeltoid and sub coracoid bursitis.
Mild AC arthrosis and degeneration of the superior posterior superior labrum. We discussed surgical and non-surgical treatment and the patient refused the surgery and wanted to give the conservative medication. Tramadol was prescribed for pain management.
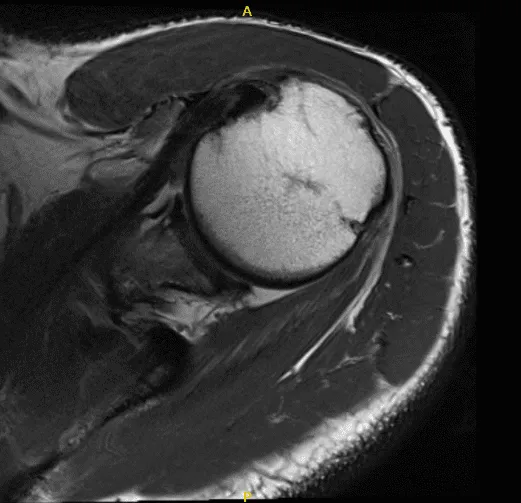
MRI of left shoulder
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, nonhealing, repeat surgery, injury to adjacent nerves and vessels, rehabilitation and stiffness, need for manipulation among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where a supraclavicular block was given. General anesthesia was induced. The patient was turned into the right lateral position with the left shoulder up. Axillary roll was put. Bean bags were used for positioning. All the bony prominences were well padded.
The left upper extremity was prepped and draped aseptically in the usual fashion. Preoperative antibiotics were given in the form of Ancef 2 g. Time-out was called. Posterior entry portal for the shoulder was made and the scope was entered through the glenohumeral joint.
Entry to the anterior portal was made using a spinal needle through the rotator interval and cannula was inserted. Probe was used by examining the shoulder and found to have mild osteoarthritis, grade 1 to grade 2 osteoarthritis of the glenoid center.
There was partial tearing of the subscapularis, which was debrided. There was mild tendinitis of the biceps tendon and nothing was done for that. Complete rotator cuff tear was seen in the supraspinatus and Infraspinatus of the shoulder. There was fraying of the glenoid labrum, which was debrided using the shaver.
The examination of the shoulder was normal. The scope was entered through the anterior portal, findings. The scope was entered into the subacromial space.
Examination showed bursitis, which was debrided using the shaver. Big tear of the supraspinatus and infraspinatus was found. The tear was extending up to the biceps tendon.
The shoulder was thoroughly irrigated and drained. Closure was done using #3-0 Nylon, ABD and tape. The patient was extubated and moved to the recovery unit in a stable condition.
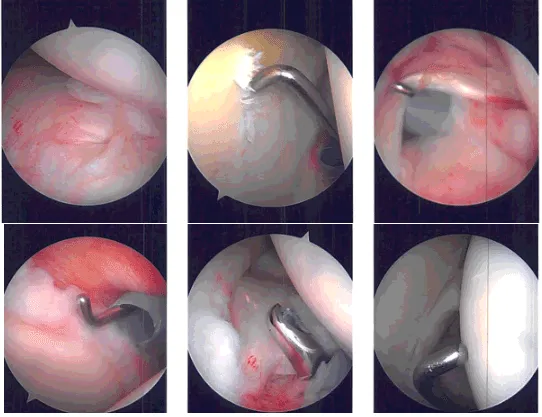
Intraoperative Arthroscopy Images
After a week post-operative, a patient came into the office to discuss the treatment options. We have decided to proceed with formal physical therapy as well as a home exercise program for the rehabilitation of her shoulder.
Stitches were removed. Patient will continue the ice and elevation for it helps with her condition. Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
