A shattered bone’s fragments are surgically fixed together during an open reduction and internal fixation (ORIF). To keep the shattered bone together, screws, plates, sutures, or rods are employed.
Due to the fibula’s function in maintaining ankle stability, you might be recommended to use crutches instead of putting weight on the injured leg until the bone heals.
Patient was in our office with complaints regarding pain on the right ankle joint, right wrist, and left wrist. She fell on ice and landed on the right side of her body. For location, the patient reported right. For quality, he reports aching. For severity, he reported moderate. For previous surgery, he reports none.
We discussed treatment options and the opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, failure of implant, need for repeat surgery, arthritis, systemic complications including blood clot, cardiac, pulmonary, neurological complications including death, the patient understood and signed an informed consent.
The patient was brought to the operating room where she was placed on a well-padded operating table. General anesthesia was induced. Preop antibiotic was given. High thigh tourniquet applied. A bump was applied onto the hip. The right leg was put on elevation under bedsheets.
Her right lower extremity was prepped and draped aseptically in usual fashion. C-arm was brought in. Tourniquet was elevated after application of Esmarch. Fracture was seen under fluoro again.
A distal fibular incision was given and with sharp dissection the bone was reached. The fracture could be seen. The fracture was opened and irrigated and drained. The fracture was reduced and held with a lobster clamp.
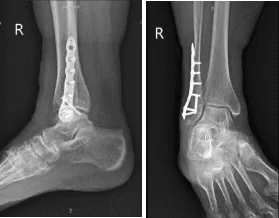
An interfragmentary screw was planned and a 3.5-mm interfragmentary screw was inserted after drilling across the fracture site. Distal fibular plate was put and held by olive wires and checked under fluoro and found to be in acceptable position.
X-ray Right ankle minimum 3 views
The fracture was well reduced. The distal fibular plate was fixed to the fibula with the use of a combination of locking and nonlocking screws. Final picture was taken under rotational fluoroscopy and found to be in an acceptable position. The wound was irrigated and drained.
Closure was done in layers using #0 Vicryl, # 2-0 Vicryl, #3-0 Monocryl followed by Dermabond and 4×8. Webril and posterior splint was applied and applied. The patient was extubated and moved to recovery in a stable condition. Tourniquet was released after the application of the splint.
The patient was seen for post operative check up after three weeks with X-ray results that showed healing distal fibula fracture status post ORIF, without evidence of hardware complications. Comparison to prior posttraumatic/postoperative radiographs recommended.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
