The hip is a ball-and-socket joint, and in this surgery both worn-out parts are replaced. Here, the damaged ball at the top of the thigh bone and the worn socket in the pelvis are swapped for smooth, low friction, artificial parts. The goal is to relieve pain and get people moving comfortably again after arthritis or injury has made walking, sitting, or standing difficult.
Most people who have it experience major pain relief and a return to normal activities, and modern implants commonly last 20 to 30 years.
This page covers the conditions it treats, when to consider it, what the surgery and recovery involve, and the risks.
What condition does this treat:
This treats a hip joint that’s been badly damaged, usually by arthritis. Most patients are between 50 and 80, though it can help people of any age. The common causes are:
- Osteoarthritis — the age-related wearing away of the smooth cartilage that cushions the joint. This is the most common reason.
- Rheumatoid arthritis — a condition where the immune system attacks and inflames the joint.
- Avascular necrosis — bone death caused by a loss of blood supply, often after an injury or certain medications.
- Post-traumatic arthritis — arthritis that develops after a hip injury or fracture.
In all of these, the joint’s cartilage breaks down until bone rubs directly on bone, which causes pain and limits movement.
When should you consider surgery:
The most common signs that a hip may need replacing include severe hip pain during everyday activities like walking or sitting, stiffness that makes it hard to bend or move the leg, pain even at rest (especially at night). Patient will also have trouble with basic tasks like putting on shoes or getting in and out of a car.
Surgery is usually considered only after conservative treatments have been tried and have not provided symptom relief. Non-operative treatment incudes medication, physical therapy, and joint injections.
To confirm what’s going on, doctors typically do a physical exam and imaging such as X-rays. Sometimes we will also conside MRIs, CTs, or bone scans in more complex cases.
Part of that workup is ruling out other problems that can mimic hip arthritis, like bursitis, sciatica, a torn rim of socket cartilage, or bony vascular problems.
What happens during surgery:
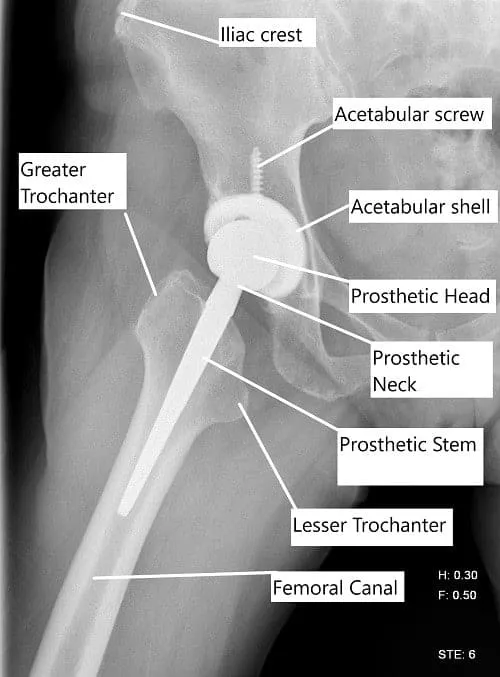
The surgeon removes the damaged ball at the top of the thigh bone and the worn surface of the socket, then puts in artificial parts. This includes a stem placed into the thigh bone, a new ball that attaches to the stem, a cup fitted into the socket (sometimes held with small bone screws), and a smooth plastic liner inside the cup so the joint glides easily.
There are a few variations in how this is done, and your surgeon chooses based on your situation:
- Cemented vs. cementless — the parts are either held with bone cement or designed so your bone grows into them and grips them naturally.
- Anterior vs. Posterior vs Lateral — the surgeon reaches the joint from the front or the back.
- Minimally invasive — a smaller incision, used in select patients.
{kind=link}
Surgeons often use trial parts to check the fit and, in some cases, a live X-ray to confirm placement before locking in the final implant.

Femoral Prosthetic Component
What does recovery look like:
Most people stay in the hospital for one to three days. Occasionally, healthy patients can go home the same day if their pain is controlled.
Pain is managed with a mix of medications, injections, and therapies. Physical therapy usually starts right away to rebuild movement and strength.
Most people recover fully within three to six months, though it can take longer for some. Walking is started day 1 after surgery. Most patient have a pain free hip by 6 weeks post op. Driving can be resumed around 6 weeks post op. Most seditary work can be resumed at 4 weeks, and heavy manual labor closer to 12 weeks post operatively.
As the new hip heals, low-impact activities like walking, swimming, and cycling are encouraged. High-impact activities like running are discouraged, since they wear the new joint out faster.
With good care, the implant commonly lasts 20 to 30 years.
What are the major risks and complications:
Serious complications are uncommon, but no surgery is risk-free. The main ones are:
- Infection, at the incision or deeper around the implant.
- Blood clots in the leg, which can be dangerous if one travels to the lungs.
- Dislocation, where the new ball slips out of the socket — more likely if the parts aren’t well aligned.
- A small difference in leg length after surgery.
- Implant loosening over time, which can eventually require a repeat (revision) surgery.
Your surgeon will discuss how these apply to your specific case.
What if you don’t have surgery:
Surgery is a choice, not a requirement. Many people manage hip arthritis for a long time with medication, physical therapy, and injections. Those are sensible first steps and worth trying.
But arthritis doesn’t reverse itself. it tends to get worse with time and use. The joint tends to keep wearing down, so for many people the pain and stiffness slowly get worse. Everyday activities become harder over time. Non-surgical care can ease the symptoms but doesn’t repair the underlying damage.
The right time for surgery is different for everyone, and it’s a decision to make with your doctor based on how much your hip is affecting your daily life and quality of life.
I typically have two main criteria. If the pain is severe enough to undergo a major operation, then it is time to consider replacement. It is considered a major operation. The second criteria is that you are committed to the 2-3 months of intense rehab that is required to recover after such a surgery. These are the patients that are content with their surgery.
Insurance & Cost
Total Hip Replacement Surgery at Complete Orthopedics is covered by Medicare and most major insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), as well as most workers’ compensation and no-fault insurance plans. Your out-of-pocket cost depends on your specific plan, deductible, and the medical necessity criteria that apply to your case.
Call our billing team at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs. For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
Dr. Athar’s perspective on Total Hip Replacement:
“Undergoing a total hip replacement is a monumental decision and is one that I do not take lightly. It is considered major surgery. My philosophy is less focused on the X-ray and more based on your symptoms. It’s about the life that X-ray is representing.
I typically recommend surgery only when we’ve reached a quality-of-life crossroads. If you’ve exhausted conservative options like physical therapy, injections, braces, medication, supplements, and alternative treatments, then this major surgery is something we should consider.
If you’re still finding yourself sitting on the sidelines of your own life, then you’ve reached the critical threshold. I would like to explain that there are two major commitments when undergoing a hip replacement.
Firstly, we have to commit to the risks involved in the surgery. These complications are rare but can be devastating when they happen. You have to be comfortable with the risk.
Secondly, you have to have commitment to the exhaustive rehab (several months) after the replacement surgery. It is just as important as the surgery itself. If you can commit to these two things, then I can help rebuild a functional hip for you.
When we talk, I won’t just show you bone-on-bone arthritis. I’ll ask you what you can’t do today that you want to do tomorrow. Whether it’s playing a round of golf without a week of recovery or simply walking down the stairs to breakfast without a wince.
You set the direction of this decision. I view my role as an educator, laying out the benefits and pitfalls of surgery versus continued management so you can make a choice that feels right for your timeline.
A successful outcome is deeply personal and goes far beyond a straight leg on an exam table. To me, a good result means regaining your independence and, ideally, forgetting about your hip entirely.
Success is the moment you realize you went the whole afternoon without thinking about your joint.
My fellowship training in reconstructive surgery taught me that precision in the OR is the baseline, but the way that training truly benefits you is in the predictability of your recovery.
I chose this specialty because orthopedics offers the unique ability to fix a mechanical problem and provide a tangible return to health. Seeing a patient return to the hobbies or jobs they love is why I do this.
We aren’t just replacing a joint; we are restoring your ability to engage with the world on your own terms.”
Do you have more questions?
What are the different types of materials used in total hip replacements, and how do they differ in terms of durability and performance?
Total hip replacements can be made of various materials, including metal, ceramic, and plastic. Each material has its advantages and considerations in terms of durability, wear resistance, and compatibility with the patient’s anatomy. We surgeons decide what is the optimal implant selection based on your specific situation
How does age affect the decision to undergo total hip replacement surgery, and are there any age restrictions for the procedure?
Age is a consideration in the decision-making process for total hip replacement surgery, but there are no strict age restrictions. The decision is based on factors such as the patient’s overall health, functional status, and the severity of hip joint disease.
Can individuals with certain medical conditions, such as diabetes or heart disease, still undergo total hip replacement surgery?
Yes, individuals with certain medical conditions can undergo total hip replacement surgery, but their medical status will be carefully evaluated to optimize safety and minimize risks during the procedure.
Can total hip replacement surgery relieve all symptoms of hip pain and dysfunction, or are there limitations to its effectiveness?
Total hip replacement surgery can significantly alleviate symptoms of hip pain and dysfunction in most cases, but it may not completely eliminate all symptoms, especially if there are underlying issues such as nerve damage or muscle weakness.
What type of anesthesia is used for total hip replacement surgery, and how is pain managed during and after the procedure?
Total hip replacement surgery is commonly performed under general anesthesia or regional anesthesia (such as spinal or epidural anesthesia). Pain during and after the procedure is managed with a combination of medications, including local anesthetics, opioids, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Can individuals with a history of hip surgeries or hip trauma still undergo total hip replacement surgery, or are there contraindications?
Individuals with a history of hip surgeries or hip trauma may still be candidates for total hip replacement surgery, depending on the extent of previous interventions, residual hip function, and the presence of any complicating factors.
What are the potential complications associated with anesthesia during total hip replacement surgery, and how are they managed?
Complications of anesthesia during total hip replacement surgery may include allergic reactions, respiratory issues, blood pressure changes, and adverse drug interactions. Anesthesia is carefully monitored by anesthesiologists, and appropriate interventions are implemented to manage any complications that arise.
How does total hip replacement surgery affect mobility and independence in daily activities, especially in older adults?
Total hip replacement surgery can significantly improve mobility and independence in daily activities for older adults by reducing pain, increasing joint function, and restoring quality of life.
What are the dietary recommendations before and after total hip replacement surgery to promote healing and recovery?
Before and after total hip replacement surgery, patients may be advised to follow a balanced diet rich in protein, vitamins, and minerals to support tissue healing, strengthen muscles, and promote overall health.
Can total hip replacement surgery be performed simultaneously on both hips, or is it typically staged?
Total hip replacement surgery can be performed simultaneously on both hips in select cases, but it is more commonly staged, with each hip undergoing surgery separately to minimize the risk of complications and optimize recovery.
Are there any specific exercises or physical therapy programs recommended before and after total hip replacement surgery to improve outcomes?
Yes, preoperative exercises and physical therapy programs may focus on strengthening muscles, improving joint flexibility, and optimizing overall fitness to enhance surgical outcomes and facilitate postoperative recovery.
Can total hip replacement surgery be performed using robotic-assisted techniques, and what are the potential benefits of this approach?
Yes, total hip replacement surgery can be performed using robotic-assisted techniques, which may offer advantages such as improved accuracy, precision, and personalized implant placement, potentially leading to better outcomes and faster recovery for patients.
How does the experience and expertise of the surgeon impact the outcomes of total hip replacement surgery?
The experience and expertise of the surgeon play a significant role in the outcomes of total hip replacement surgery, with skilled surgeons often achieving better results in terms of implant longevity, functional improvement, and patient satisfaction.
Can total hip replacement surgery be performed in outpatient settings, or is it typically done in hospitals?
Total hip replacement surgery is usually performed in hospitals, where patients can receive comprehensive care, including preoperative evaluation, surgical intervention, anesthesia, postoperative monitoring, and rehabilitation services. However, some less complex cases may be suitable for outpatient or ambulatory surgery centers.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.

