Acromioplasty, also known as shoulder subacromial decompression, is a surgical treatment used to treat shoulder impingement, a common problem that results in discomfort and weakness in the shoulder when you lift your arm over your head.
A ruptured tendon in the shoulder can be repaired surgically with rotator cuff repair. Shoulder arthroscopy, which employs smaller incisions, or a big (open) incision might be used for the operation. Several muscles and tendons come together to create a cuff around the shoulder, called the rotator cuff.
Common treatment for tendinopathy of the long head of the biceps brachii (LHB) is biceps tenodesis. Partial-thickness LHB tears, tendon subluxation with or without subscapularis tears, and unsuccessful conservative therapy of bicipital tenosynovitis are examples of indications.
If you experience any of the following signs of shoulder discomfort or are unable to move your shoulder normally, you should get in touch with an orthopedic surgeon. You may experience shoulder dislocation. There is obviously something wrong with your shoulder joint.
A 49-year-old patient was in our office with complaints regarding his shoulder pain following an accident. We injected the left shoulder but had no relief. We discussed treatment options and the patient opted for surgical management.
We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, possibility of repeat injection, possibility of shoulder pain and need for cortisone injections among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. He was turned in the right lateral position so that the shoulder was up. The left shoulder was prepped and draped aseptically in the usual fashion.
The left shoulder was put into 40 degree of abduction and 10 degrees of flexion with the use of called. Perioperative antibiotics given. Anterior portal was made posteriorly through a soft shoulder sport. The Glenohumeral joint was reached and entry into the anterior portal was made using a spinal needle.
The glenohumeral joint was examined. Subscapularis, suprascapularis, intrascapular, and biceps tendon were intact. There was no arthritic change in the glenohumeral joint. There was fraying of the glenoid labrum, which was cleaned using a shaver. There was no articular side rotator cuff tear.
The scope was entered into the subacromial region. Bursitis was present. The shaver was used to clean off the bursitis. There was some subacromial spurring which was cleaned by using bur and doing subacromial acromioplasty. The rotator cuff was examined, and this was found to be intact.
There was arthritis in the AC Joint. The decision for distal clavicular excision was taken. The distal clavicular excision was performed using the bur from the posterior portal as well as the anterior portal.
A centimeter of distal clavicle was excised. Dressing was done using Xeroform, 4 x 4, ABD, and tapes. The patient was put in a shoulder sling. The patient was extubated and moved to recover in a stable condition.
The patient visited our office again with complaints regarding pain in both of his shoulders for months. He had undergone arthroscopic surgery on the left shoulder a few weeks ago. He has no pain in the left shoulder.
He came into our office with recurrent right shoulder recurrent pain which has not been getting better. The patient was weak in his rotator cuff muscles. The patient presented an MRI result and showed that it was normal but there was a high suspicion of rotator cuff tear.
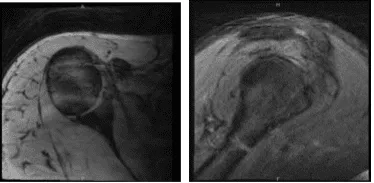
MRI-3T Right Shoulder non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed infection, bleeding, nonhealing, need for repeat surgery or repair, injury to adjacent nerves and vessels, systemic complications among others. The patient understood and signed informed consent.
The patient was taken to the operating room where general anesthesia was induced. A supraclavicular block was given in the holding area. The patient was put in the left lateral position with the right shoulder up. An axillary roll was applied. All bony prominences were well-padded.
He was held in place with a bean bag. Preop antibiotics were given. The right upper extremity was prepped and draped aseptically in the usual fashion. A posterior entry portal was made through a soft spot. The Glenohumeral joint was reached. Debridement was done with a shaver.
There was a partial articular sided rotator cuff tear. The decision was made to repair the rotator cuff. Debridement of the rotator cuff edges was done. Bony attachment was decorticated and prepped using a burr. The path for the SwiveLock was checked using a spinal needle followed by an incision.
The SwiveLock was inserted after punch insertion. Once the anchor was in place, one limb of the satire was retrieved using a bird beak through the medial rotator cuff the scope was entered into the subacromial space.
The sutures were visualized. The suture was knotted. A good repair was achieved. There was no subacromial bursitis or fraying. The AC joint looked good. Final pictures were taken and saved.

Intraoperative Arthroscopic Images
The shoulder was thoroughly irrigated and drained. Closure was done using 3-0 nylon. shoulder immobilizer. in stable condition. Dressing was done. The patient was put in a shoulder immobilizer. The patient was extubated and moved to recovery.
The patient came back to our office. He underwent right shoulder rotator cuff repair with me four months ago. He started having pain in his right shoulder, especially in the anterior part. The patient did physical therapy, but the pain did not relieve.
An MRI result was presented which showed biceps tenodesis and possible tear in the rotator cuff. Evidence of prior rotator cuff repair with suture anchor in the greater tuberosity. However, findings compatible with a recurrent tear of the supraspinatus at least moderate severity.
Low-grade partial thickness tear of the subscapularis tendon. Biceps tendinosis and tenosynovitis without tears. Findings suggesting adhesive capsulitis. Small tear at the base of the anterior labrum. Mild bursitis.
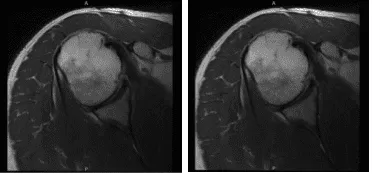
MRI-3T Right Shoulder non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, nonhealing, repeat surgery, rehabilitation, and stiffness, among others. The patient understands and signed informed consent.
The patient was taken to the operating room where general anesthesia was induced. The right upper extremity was prepped and draped aseptically in a usual fashion. Preop antibiotic was given. Incision was given for the posterior entry portal and arthroscope entered.
There was some fraying of the labrum, which was debrided. No rotator cuff tear could be seen on the surgical site. The Glenohumeral examination also showed inflammation of the biceps tendon with fraying. Biceps tenotomy was performed on the joint with a plan for doing a subpectoral biceps tenodesis. The scope was entered into the subacromial space.
Examination of subacromial space showed bursitis and thickened bursa, which was removed. Satisfactory acromioplasty was already there. The AC joint was intact and no inflammation was seen and so no intervention was done there.
There was superficial fraying, then 50% deep tear of the supraspinatus was seen. A decision was made to use a regeneten patch. Tear was debrided and Patch was inserted through the lateral entry portal and placed over the frayed area.
It was tacked to the rotator cuff using PLA staples x 5. The lateral part of the patch was tacked to the greater tuberosity using PEEK staples x 2. It was found to be in a stable condition. Final pictures were taken and saved.
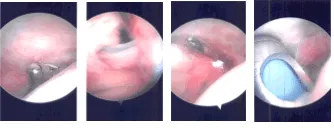
Intraoperative Arthroscopic Images
The scope was removed, and the arm was removed from traction. A 3 cm anterior axillary Fold incision was given for subpectoral fascia was brought in the line of biceps tenodesis incision. Subpectoral dissection led to the tendon of the long head of the biceps. The biceps tendon was delivered.
The suture of the tendon using fibrecinch was performed. From the myotendinous junction proximally, a drill hole was made for the button insertion. The tendon sutures were put on the Endo button and the button was inserted through the drill hole and tightened.
The suture was passed to the tendon again and tied onto itself. The unicortical PEEK screw was not used as it was not stable.
The wound was thoroughly washed and closed in layers using #0 Vicryl, #3-0 Vicryl followed by #4-0 Monocryl. The incisions are closed using nylon #3-0. The wound was infiltrated with 0.5% lidocaine x10 cc.
The wounds were dressed using 4×8 followed by ABD and dressing was performed. Sterile dressing was applied. The patient was extubated and was moved to recover in stable condition.
We have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. The patient did well after the surgery and continued physical therapy. The patient checked in for a follow up visit after a month and saw significant improvement in his shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 24, 2025.
