Shoulder arthroscopy can relieve excruciating signs and symptoms of a variety of conditions that harm the articular cartilage, labrum, rotator cuff tendons, and other soft tissues around the joint. Rotator cuff repair is one of the most frequent arthroscopic surgeries. Labrum removal or repair.
It’s possible that untreated chronic inflammation brought on by a partly torn rotator cuff tendon can proceed to a full-thickness tear and eventually to shoulder arthritis, at which time you might not be able to lift your arm above because of shoulder weakness and pain.
A 55 year-old patient was in our office with complaints regarding left shoulder pain after a fall mountain biking and falling on shoulder. His pain has not improved. For aggravating factors, the patient reported lifting.
For associated symptoms, tingling and pain with motion but reports no weakness, no numbness, no swelling, no redness, no warmth, no ecchymosis, no catching/locking, no popping/clicking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness.
For location, he reports left. For quality, he reported stabbing and throbbing. For severity, moderate.
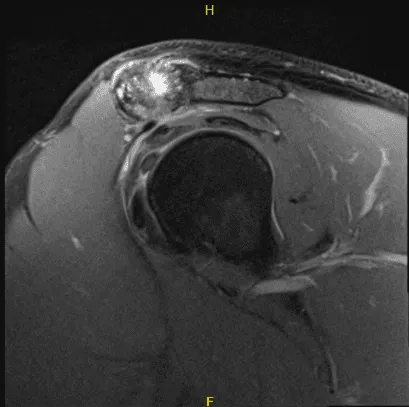
The patient presented an MRI result that showed high-grade partial-thickness articular surface tear at the supraspinatus tendon insertion. Low-grade partial-thickness articular surface tear of the distal infraspinatus tendon. Moderate AC joint arthrosis.
A small subacromial spur predisposes the patient to external impingement. Nondisplaced tear of the posterosuperior labrum. Mild subacromial subdeltoid bursitis.
Intraoperative Arthroscopy Images
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, failure of the pain to resolve, repeat tear, need for repeat surgery, systemic complications including blood clots, cardiac, pulmonary, neurological complications including death. The patient understood and signed an informed consent.
The patient was brought to the operating room where he was placed on a well-padded operating table. General anesthesia was given. Supraclavicular block was already done preoperatively in the holding area.
The patient was turned into the right lateral position with a left shoulder up. He was held in position with the use of a bean bag. All the bony prominences were well padded. Axillary roll was used. The left shoulder was prepped and draped aseptically in a usual fashion.
Preop antibiotic was given. The left shoulder was put in 45-degree abduction and flexion and on traction with 10 pounds of weight. Posterior entry portal was made through the soft spot and an arthroscope was inserted.
A medical entry portal was made with the use of a spinal needle. Examination of the glenohumeral joint showed grade 1 to grade 2 osteoarthritis changes of the glenoid fossa. Articular cartilage of the head of the humerus was intact. There was no tear in the biceps.
Labral tear could be seen along the superior aspect without involvement of the biceps anchor. Debridement of the labrum was done with the use of a shaver. Articular site high-grade partial thickness tears could be seen in the supraspinatus.
Debridement was done and tagging was done with the use of PDS suture. Rest of examination of the glenohumeral joint was intact. Pictures were taken and saved. The arthroscope was inserted into the subacromial region. Shaver was introduced from anterosuperior portal. Debridement of the bursa of the subacromial space was performed with the use of a shaver.
The rotator cuff was examined in the region of the PDS and found to have near complete tearing of the supraspinatus. A shaver was used to complete the tear. Debridement of the tear and the head of the humerus was performed in preparation for the repair.
Further accessory portals were made for planning of the repair. was put into the head of the humerus followed by a tap and 4.75 mm Regenesorb Healicoil anchor from Smith & Nephew with portals was inserted.
The suture was brought out sequentially from the accessory portal and loaded on the first path and passed through rotator cuff sequentially from the posterior to anterior avoiding the biceps. The sutures were tied onto each other to achieve a good repair.
A lateral row was planned and followed by insertion of the sutures on the multifix was done to complete the lateral repair. The AC joint was found and debrided with the use of a shaver.
A plan from distal clavicle excision was performed, was made and 6.0 bur was used to excise the articular surface of the AC joint. About a centimeter of the distal clavicle was excised to the posterior as well as anterior superior portal. Final pictures were taken and saved.
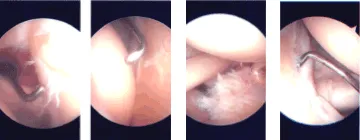
Intraoperative Arthroscopy Images.
Irrigation of the shoulder was done and drained. Closure was done with the use of # 3-0 nylon. Dressing was done with the use of 4 x 8s, ABD, tape. The patient was put in a shoulder immobilizer and after extubation, moved to recovery in a stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder.
The patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
