The distal clavicle excision surgery is used to relieve shoulder discomfort and impairment brought on by arthritis or impingement by removing the outside portion of the clavicle (collarbone).
Untreated bone fractures can lead to either a delayed or non-union of the bone. In the first scenario, the bone doesn’t mend at all, therefore it will continue to be shattered. As a result, over time, swelling, soreness, and discomfort will only become worse.
A 45 year-old patient visited our office with complaints regarding right shoulder pain due to a car accident. She has been trying physical therapy and anti-inflammatory medications, but had no relief.
She presented MRI for the right shoulder and showed diffuse tendinosis with a partial thickness tear of the anterior insertional footprint of the supraspinatus tendon. Diffuse tendinosis of the infraspinatus with an interstitial partial delamination tear. Subscapularis tendinosis.
Diffuse superior labral tear/SLAP tear. Tear of the posterior-inferior labrum with partial detachment. Inferior capsular sprain versus adhesive capsulitis. Small effusion. Focal subchondral cyst and focal cartilage defect along the posterior glenoid rim with early subchondral wear pattern.
Subacromial subdeltoid bursitis. Hypertrophic change of the AC joint with Grade I capsular sprain. Edema in the distal clavicle and the acromion which may represent contusion or stress reaction. Narrowing of the subacromial space. Bone marrow edema at the greater tuberosity compatible with bone contusion.

MRI Scan of the right shoulder
The patient also presented an Xray results and showed normal right shoulder radiographs.

Right shoulder X-ray
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections, and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to anesthesia, infection, damage to nerves and blood vessels, blood loss, blood clots, and even death were discussed at length.
We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
We talked about the possibility of not being able to alleviate all of the discomfort. Also, I explained there is no guarantee all the function and strength will return. The patient also understands the risks of re-tear or failure to heal.
The patient understands implants may be utilized during this surgery. The patient expressed understanding of these risks and has elected to proceed with surgery. We have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome, and post operative protocol.
The patient was taken to the operating room where a supraclavicular block was done. General anesthesia was induced, and the patient was intubated. She was turned in a left lateral position with the right shoulder up in a floppy lateral position and held with a beanbag.
All the bony prominences were well padded. Axillary roll was inserted. Preoperative antibiotic was given. The right shoulder was prepped and draped aseptically in the usual fashion. A posterior entry portal was made through the soft spot.
The arthroscope was inserted into the glenohumeral joint where examination showed fraying of the lateral part of the subscapularis tendon, fraying of the anterior and posterior labrum, grade 1 to grade 2 lesion of the cartilage of the glenoid head, fraying and partial tearing of the rotator cuff on the articular side.
Debridement was done with the use of shaver for the glenoid labrum, subscapularis tendon, articular cartilage of the humeral head as well as the rotator cuff. The arthroscope was inserted in the subacromial space. Examination showed partial freeing of the rotator cuff along the supraspinatus.
There was lateral anterior spurring of the acromion as well as AC arthritis. Shaver followed by a Coblation wand was used to clear up the acromion as well as the AC joint.
Repair of the rotator cuff tear was performed with the use of a small Regeneten implant, which was put in place with the use of multiple tacks through lateral and the accessory superior portal. Pictures were taken for the draft.
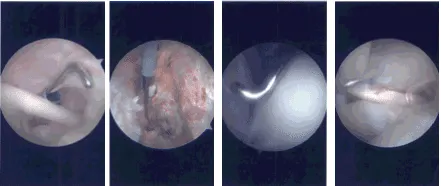
Intraoperative Arthroscopy Images
Acromioplasty was performed with the use of a #6-0 bur followed by distal clavicular excision by removing about 1 cm of the distal clavicle through the posterior and followed by the anterior portal. All the pictures were taken and saved.
The shoulder was thoroughly irrigated and drained. Closure was done with the use of #3-0 nylon. Dressing was done with the use of 4 x 4, ABD, tape. The patient was extubated and put in a shoulder sling and moved to Recovery in a stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 24, 2025.
