For the following shoulder issues, arthroscopy may be advised: ligaments or a torn or broken cartilage ring (labrum). Shoulder instability is characterized by a loose shoulder joint that moves about excessively or dislocates (slips out of the ball and socket joint). an injured or torn biceps tendon.
A 40-year-old patient was in our office with complaints regarding right shoulder pain. This is from a traffic accident. He has undergone nonoperative treatment in the form of physical therapy and anti-inflammatory medications. For aggravating factors, standing, lifting, and pushing/pulling.
For associated symptoms, weakness, numbness, tingling, swelling, redness, popping/clicking, tender to the touch, and pain with motion but reports no redness, no warmth, no ecchymosis, no catching/locking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, and no change in bowel/bladder habits.
For quality, aching, numbness, and tingling. For severity, severe. For alleviating factors, he reported nothing helps. For previous surgery, none.
The patient presented MRI results that have shown small full-thickness tear of the distal supraspinatus tendon at its insertion measures 1.3 x 1.5 cm. Background tendinosis and attrition of the torn supraspinatus tendon. Tendinosis of the superior distal subscapularis tendon.
No rotator cuff muscle atrophy. Mild tendinosis, intra-articular long head of the biceps tendon with mild tenosynovitis. Tear of the posterosuperior labrum. Small subacromial subdeltoid bursitis communicates freely with small joint effusion. Mild osteoarthritis of the AC joint.
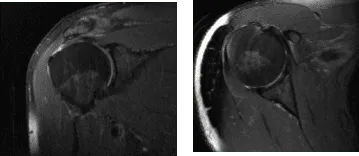
MRI Right Shoulder Non-contrast
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections and surgical options. I also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to infection, stiffness, damage to nerves and blood vessels, blood loss possibly requiring transfusion, blood clots, persistent or worsening pain, loosening or failure of implants, instability, tingling or numbness, anesthesia and systemic complications including cardiac, pulmonary, neurological complications and even death were discussed at length.
I also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
I talked about the possibility of not being able to alleviate all the discomfort. Also, I explained there is no guarantee all the function and strength will return. I discussed the type of implants that may be utilized during this surgery. The patient expressed understanding of these risks and has elected to proceed with surgery.
I discussed the patient’s medications and allergies and the possible need for medical and other clearances if needed. I have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome and post operative protocol.
The patient was taken to the operating room where a supraclavicular block was given. The patient was sedated and placed in the left lateral position with the right shoulder up. All of the bony prominences were well-plated.
The right shoulder was prepped and draped in the aseptic usual fashion and put in traction with flexion and abduction with a 15 pound weight. Preoperative antibiotic was given. An anterolateral portal was made through the posterior soft spot. The arthroscope was inserted into the glenohumeral joint.
A portal was made with the use of a spinal needle. Examination of the glenohumeral joint showed biceps labral tear involving the biceps anchor, SLAP tear, rotator cuff tear full thickness. There was no damage to the cartilage. Debridement of the labrum and biceps tenotomy was performed with the use of a punch.
The arthroscope was inserted into the subacromial space and the shaver was introduced through the anterior portal and debridement of the bursa was done in the subacromial space. There was a large rotator cuff tear which was debrided. An acromioplasty was performed to remove the acromial spur and make space for the rotator cuff repair.
There was AC arthritis which also caused pain and procedure was done by removal of about 1 cm of the distal clavicle. Attention was diverted towards the rotator cuff. Debridement of the footprint for the rotator cuff was done with the use of a bur.
A triple blade box screw bio clavicle Arthrex anchor was used and inserted. The sutures were passed sequentially in a horizontal mattress fashion. The middle suture was lost so fiber tape was passed in a horizontal mattress fashion. The anterior and posterior sutures were tied to each other.
The sutures from the anterior posterior along with the horizontal mattress of the fiber tape were used and a lateral repair was performed with the use of 4.7 SwiveLock. Good reduction of the rotator cuff was achieved. The wound was thoroughly irrigated and drained.
Now the arm was removed from the traction and put in flexion and external rotation. A 3 cm incision was made along the inferior portion of the pectoralis major. The deltopectoral fascia was cut in the line of incision and dissection was done between the pectoralis major and the deltoid superficially on the deep side and Hohmann was inserted laterally.
Retraction was done beginning with the Army-Navy. The bicipital groove was reached and the biceps was delivered. Hemostasis was achieved and the bicipital groove was clean. The biceps fiber loop was used to do a whipstitch suture on the biceps starting at the musculotendinous junction. Excessive biceps were removed.
Drilling was done in the bicipital groove bicortically followed by remaining unicortically with a 7 mm drill and a 7.5 mm rearner. The biceps was fixed with the use of a button, fixed bicortically and clipped. The suture was tied onto the tendon.
Finally a suture was passed through the 7 mm button, it was a unicortical fixation. The sutures were cut. The wound was thoroughly irrigated and drained. Closure was done in layers with O Vicryl, 2-0 Vicryl for the biceps tenodesis and 3-0 for the shoulder incision.
Dressing was done with the use of 4 x 8s, EBD, tape. The patient’s arm was put in a shoulder immobilizer. The patient was recovered from anesthesia and brought to the recovery room in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
