The wrist joint is a distal upper limb condyloid synovial joint that connects and acts as a transition point between the forearm and hand. A joint that can move in flexion, extension, abduction, and adduction. The wrist joint’s purpose is to provide the range of motion required to execute daily.
Patient is a 54 year-old female with a complaint of right wrist pain for almost a week now. Patient is right-handed. Patient is currently working as manager where she lifts and moves boxes apart from administrative work. The patient remembers the injury to right wrist after slipping on the driveway in the rain.
She was seen at the hospital where a splint was applied. She saw an orthopedic surgeon who manipulated the fracture and put a long arm cast, split on one side but not totally eased the pain. It is extremely severe in intensity. Patient describes the pain as sharp, stabbing, throbbing, aching, burning.
The pain is constant, and does disturb sleep. The pain is associated with swelling. She also informs me of pain in her wrist with tingling and numbness in the index finger on the right hand from the past.
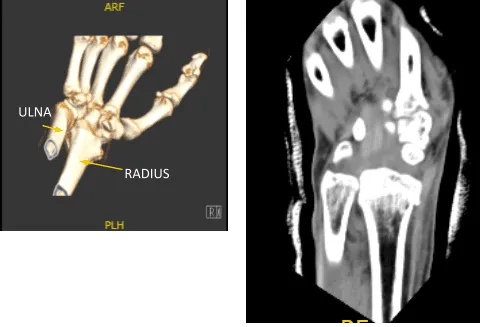
Xray were presented found comminuted impacted volarly angulated and volarly displaced intra-articular fracture of the distal radius. However, do not see any significant joint incongruity or step-off. There is ulnar plus variance. Minimally displaced fracture through the base of the ulna styloid. There is soft tissue swelling and joint effusion.
We discussed treatment- surgical and non-surgical. The patient opted to proceed with surgical management. We discussed the risks and complications of surgery including bleeding, infection, nonunion, malunion, injury to adjacent nerves and muscles, complex regional pain syndrome and others. Patient signed consent.
General anesthesia was induced into the patient and intubated. The long arm splint was removed and draped in the aseptic condition The tourniquet was applied on the upper arm and raised by 250 mmHg. A surgical incision was marked along the FCR.
The anterior sheath was opened, the pronator quadratus was erased from its radial most margin. The fracture site was opened, manipulated and reduced and held with K-wires. Distal radial plate was put over the distal radius and fixed. be with olive wires.
C-arm images were taken and manipulated to be in the correct position. Finding The plate in appropriate position, fixation of the distal radius performed using locking and nonlocking screws distally and proximally.
Final images were taken and saved. The wound was washed. Closure of the wound was done in layers. Marcaine 0.5%, 6 cc were used for locales. The skin was closed with Monocryl #4-0. A short-arm splint was applied. Shoulder sling was given. The patient was extubated and moved to the postoperative care unit in a stable condition.
After two weeks, the patient checked in with a presented Xray and saw that osseous and metallic elements are in good alignment. Patient is still in splint but not taking any pain medications. In 4th week’s post operation, observed plate fixing the distal radius is again noted with screws holding the plate in good position.
In the 6th week, splint was discarded. Finally, on her 8th week’s post operative follow up, the patient is non tender to palpation along the wrist joint line distal to radius and has mild tenderness over the styloid process of ulna, and has some soft tissue swelling around the incision. The patient has no difficulty tolerating range of motion as well as stability testing.
The ROM is 40 degrees of DF and PF. The ulnar and radial deviation is also restricted at its extremes. The patient is nontender to palpation over the elbow. They have 5/5 strength distally, and are neurovascularly intact distally. There are no erythema, warmth or skin lesions present.

AP and Lateral View of Patient RT 2 weeks Post-operative

AP and Lateral View of patient RT wrist 2 weeks Post-operative
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
