Debridement is the process of clearing the area around the shoulder joint of any loose tendon fragments, thickened bursa, and other debris. The doctor can better assess the severity of the injury and decide whether to perform additional surgery by removing injured tissue from the shoulder joint region.
At the acromioclavicular joint in the shoulder, the surgeon removes the end of the clavicle during this minimally invasive treatment. The joint will decompress if this piece of bone is removed. It will aid in reducing the discomfort and range-of-motion loss brought on by arthritis or impingement.
A 31 year-old patient male presents with neck and upper and lower back pain due to MVA. He had no pain before the accident. He tried conservative management, but it did not help him.
He works for MTA and is having difficulty doing work due to pain. We discussed the treatment options including PT, MRI, Injection, surgery and we agreed to go with MRI.
MRI were reviewed and discussed; Acromioclavicular Joint: The undersurface of the acromion is curved. There is mild acromioclavicular joint arthrosis. Rotator Cuff: There is a partial-thickness tearing the superior subscapularis tendon. There is tendinosis in the supraspinatus tendon.
The infraspinatus, and teres minor tendons are intact. There is no disproportionate muscle atrophy. The rotator interval is normal. Biceps And Labrum: The long head of the biceps’ tendon is intact and maintained in the bicipital groove. The labrum and biceps labral anchor are intact. Glenohumeral Joint:
There is a physiologic amount of fluid within the joint. The articular cartilage is maintained. Bones: There is no acute fracture or osteonecrosis. There is no suspicious bone marrow edema. Bursae: There is no significant subacromial-subdeltoid bursitis.
Miscellaneous: The deltoid muscle is maintained. There is no significant axillary lymphadenopathy. The subcutaneous tissues are within normal limits. Which means the shoulder’s MRI showed that there is a rotator cuff tear along with acromial spur and AC arthritis of the right shoulder.
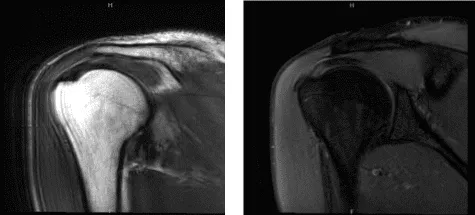
MRI Right shoulder non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed the risks and the benefits including infection, bleeding, injury to adjunct nerves and blood vessels, shoulder stiffness and rehabilitation, need for repeat surgery, need for shoulder replacement in future.
We also discussed systemic complications including blood clots, cardiac and pulmonary complications including death. The patient understood and signed the informed consent.
The patient was taken to the operating room where a supraclavicular block was given by the anesthesia team. The patient was put in the right lateral decubitus position with a bean bag. IV sedation was given. Preoperative antibiotic was given in the form of 2 g of Ancef.
The patient was put in a right lateral decubitus position with the right shoulder up and all the bony prominences were well padded. The right shoulder was prepped and draped in the usual fashion. A time-out was called. A posterior entry portal was made.
The arthroscope was inserted. A spinal needle was used to make an anterosuperior portal. A cannula was inserted through the anterosuperior portal. A shaver was introduced through the anterosuperior portal. Examination of the glenohumeral joint showed fraying of the articular side of the rotator cuff. The shaver was used to debride it.
The articular cartilage and the biceps were intact. The arthroscope was inserted through the anterosuperior portal and a thorough debridement was done through the posterior portal. The arthroscope was now entered into the subacromial space.
The shaver was inserted from the anterosuperior portal and a bursectomy was performed with the shaver. There was acromial impingement. An accessory lateral portal was made with the use of the spinal needle. The arthroscope was entered through the lateral portal.
The shaver was inserted from the posterior portal and a thorough debridement of the bursa was done. The plan for the acromioplasty was done and a 6.0 burr was inserted through the posterior portal. Acromioplasty was performed removing the acromial spur. There was AC arthritis involving the distal clavicle.
A distal clavicle excision was planned. A coblation wand was used followed by a 6.0 burr to perform the distal clavicle excision and about a centimeter of distal clavicle was excised through the posterior portal followed by the superior portal. Examination of the rotator cuff showed no tear on the bursal side.
The shoulder was thoroughly irrigated and drained. Final pictures were taken and saved. The arthroscope was removed and closure was done with the use of 3-0 nylon. Dressing was done with Xeroform, 4×4, ABD, and medical tape. The patient was awakened and moved to recovery in a stable condition.
One week after the surgery, the patient was seen in the office for his postoperative visit, no x-rays were needed. He denies fever, chills; the neck pain is resolved and the shoulder pain is improving.
After a month the patient visited the office for his follow up checkup, no x-rays were needed, he has no fever or chills, the pain in the neck has been resolved and pain in the shoulder is improving. We discussed treatment options including PT, MRI, Injection, surgery.
We agreed to go with conservative management for now. Physical Therapy will start and continue the Ice/heat, Elevation and take OTC anti-inflammatory medicines to manage pain and swelling. The patient will be back after 4 weeks for follow up checkup.
The patient did well after the surgery, from the time to time of his visits he is gradually improving. Through regular visits and continued physical therapy, the patient healed and recovered.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
