Arthroscopy is used by orthopedic surgeons to diagnose and treat knee problems. This procedure is used in conditions that affect cartilage, ligaments, tendons and other soft tissues that surround, protect and enable your knee to function properly.
A partial meniscectomy is a surgery to remove a portion of the meniscus, a crescent-shaped piece of cartilage in the knee. The meniscus acts as a shock absorber and helps to keep the knee stable. It can be damaged by an injury or by wear and tear over time. Chondroplasty is a surgical procedure that involves smoothing degenerative cartilage and trimming any unstable flaps of cartilage.
A 51-year-old female was examined with complaints of pain to bilateral knees. The patient does not recall injuring herself. She has recently started to run and exercise when she noticed it. The pain is moderate to severe in intensity.
The pain is constant, but does not disturb me while sleeping. The pain is associated with swelling, crepitus and giving way. Patients have considerable disability and have trouble in activities of daily living as well as recreation. When she rests, the symptoms get better.
Upon examination of the left knee, the patient is tender to palpation along the medial joint line, and has an effusion. Patient also has PF crepitus and tenderness on palpation along the medial and lateral PF joint line. Patellar grinding test is positive.
The patient has discomfort with McMurray’s maneuvers, and the knee is stable. They lack full flexion secondary to the effusion, but have full extension. They have 5/5 strength, and are neurovascularly intact distally.
There are no erythema, warmth or skin lesions present. On examination of the contralateral extremity, the patient is nontender to palpation and has excellent range of motion, stability and strength.
An MRI was done for diagnosis. There is a moderate-sized joint effusion and capsular inflammation. The anterior and posterior cruciate ligaments are intact. There is a complex tear of the body and posterior horn of the medial meniscus. The lateral meniscus is intact.
The quadriceps tendon and patellar tendon are intact. The medial and lateral collateral ligaments are intact. There is moderate patellofemoral chondromalacia with 15 mm partial-thickness erosion involving the medial facet of the patella. No subchondral defect or fracture identified. There is a 10 mm enchondroma in the distal metaphysis of the femur medially.
No osteochondral defect or fracture identified. On the result of the MRI, there was a complex tear of the body and posterior horn of the medial meniscus. Moderate patellofemoral chondromalacia associated with moderate-sized joint effusion and capsular inflammation.
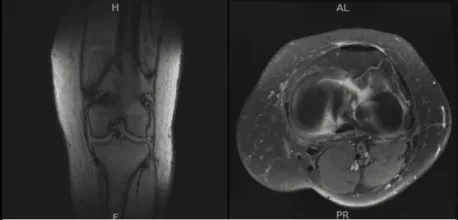
MRI-3T Left Knee Non-contrast
Upon having the diagnosis, we discussed the treatment options which includes living with the extremity as it is, organized exercises, medicines, injections and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
The patient has expressed a desire to proceed with surgery, which is a reasonable option. We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
We talked about the possibility of not being able to alleviate all of the discomfort. Also, we explained there is no guarantee that all the function and strength will return.
The patient also understands the risks of re-tear or failure to heal. The patient understands implants may be utilized during this surgery. The patient understood and signed an informed consent.
A lateral portal was made. The scope was entered and the knee was examined. There was patellofemoral arthritis. The scope was entered into the medial compartment. Medial entry portal was made using a spinal needle.
The medial meniscus was examined and found to have its margin fraying in the margin as well as degeneration of the inferior surface of the posterior horn of the medial meniscus.
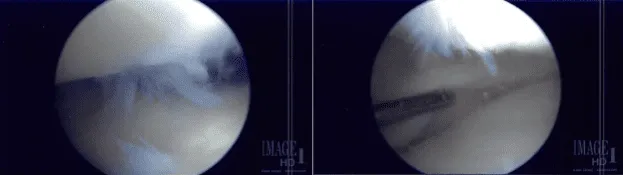
The shaver was used to remove all the fraying and balance the meniscus. The scope was introduced into the lateral compartment, where lateral meniscus was also found to be intact.
There was stage II to stage III arthritis of the femoral condyle, which was cleaned using a shaver. There was no chondral damage to the lateral femoral condyle.
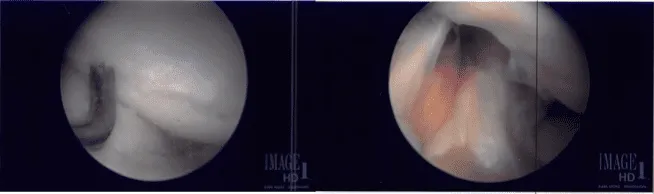
The scope was entered into the patellofemoral joint, where there was grade 3 to grade 4 arthritis and over the trochlea, grade 1 to grade 2 over the posterior surface of the patella.
Shaver and punch were used to remove all the cartilage from the trochlea as well as patella. The cartilage was balanced to a stable margin. The knee was again examined and found to be adequately debrided.
The knee was copiously irrigated with normal saline. Final images were saved. The scope was removed and the incision was closed using #4-0 nylon.
An 18-cc of Depo-Medrol mixed with 6-cc of 0.5% Marcaine was introduced into the knee joint. Dressing was done. Tourniquet was removed. The patient was extubated and moved to the postoperative care unit in stable condition.
After a week of the surgery, she has been walking with a cane or unassisted. She denies fever, chill, reinjury. She has been getting better with the pain.
She is not taking narcotics for pain medication. Patient has a regular follow up check-up in the office. The patient has undergone physical therapy which helps a lot for her full recovery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
