A 56-year-old male patient is in our office, with complaints of left knee pain for the past 3 months. He has been diagnosed with Medial Meniscus tear and osteoarthritis of the knee. He got cortisone 2 months ago, which did not help him much.
The patient takes Tylenol for pain and has no known drug allergies. He recently underwent a laparoscopic cholecystectomy. He has had no relief in her left knee pain since the last visit. His pain is worsening and is worsened with activities such as bending, walking, climbing stairs. The pain has been more on the inside of the knee.
The patient has been doing physical therapy with minimal relief of symptoms. He had earlier tried cortisone injections, visco-supplements, heat therapy without significant relief.
On examination, the patient is calm conscious cooperative, and well oriented to time place and person. The gait of the patient is steady and antalgic. Upon examination of the left knee, there is tenderness on palpation along the lateral and medial joint line and has an effusion. The medial and lateral facets of the patella are also tender on palpation.
There is a crepitus of the patellofemoral joint with a range of motion and discomfort with patella grind testing. The patient has discomfort with McMurray’s maneuvers for medial meniscus, and the knee is stable. They have a limited range of motion. Bilateral lower extremities have 5/5 strength and are neurovascularly intact distally. There are no erythema, warmth, or skin lesions present.
On examination of the contralateral extremity, the patient is nontender to palpation and has an excellent range of motion, stability, and strength.
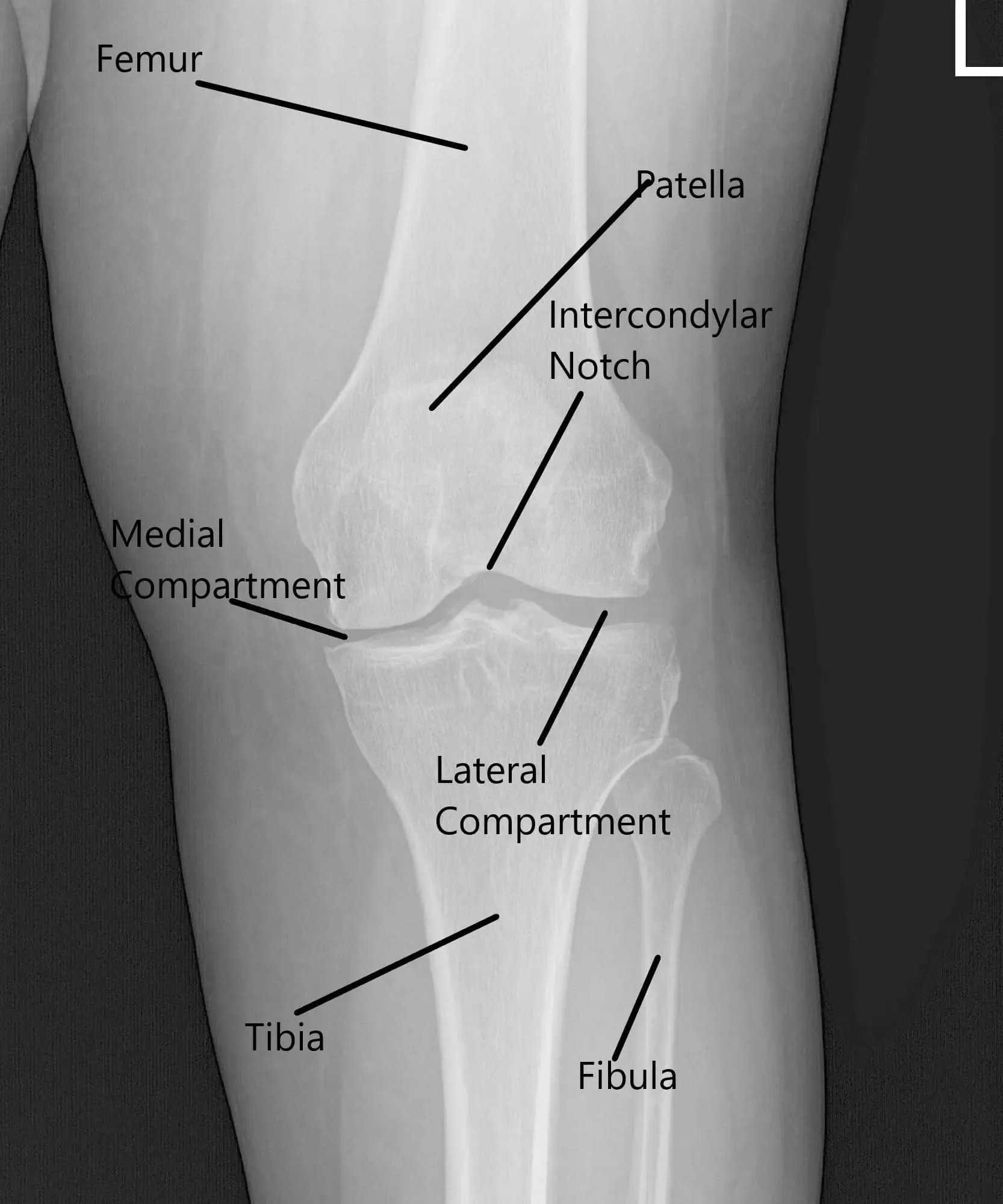
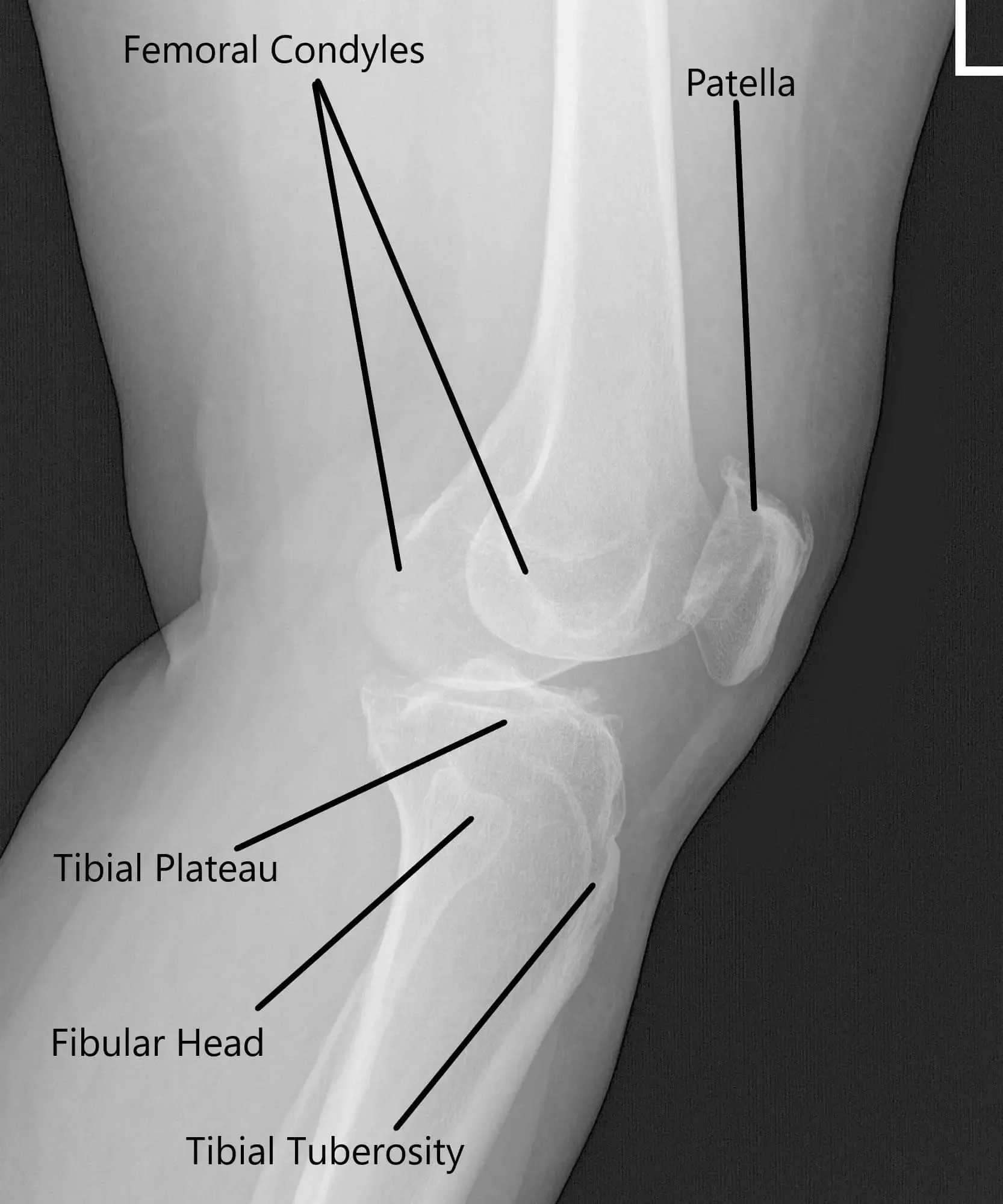
X-ray of the left knee showing AP and Lateral views.
An MRI of the left knee suggested osteoarthrosis with high-grade cartilage loss in the medial compartment and high-grade cartilage loss central trochlear cartilage with low-grade chondral loss patellar cartilage. Large radial tear posterior horn medial meniscus which is peripherally extruded. There is a loose body in the deep aspect of Hoffa’s fat pad measuring 4 mm x 8 mm.
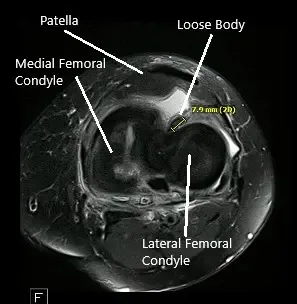
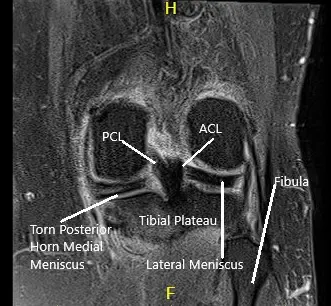
MRI of the left knee showing axial and coronal sections.
We discussed treatment options and opted for surgical management. We discussed risks and benefits including infection, injury to adjacent nerves and vessels, pain in the knee, chronic pain, complex regional pain syndrome, need for repeat surgery, need for cortisones in the future, need for knee replacement in the future, systemic complications like deep vein thrombosis, cardiac, pulmonary, and neurological complications among others. The patient understood and signed his informed consent.
PREOPERATIVE DIAGNOSES:
- Complex tear of the posterior horn of the medial meniscus left knee.
- Patellofemoral arthritis.
- Loose body along the base of the ACL.
POSTOPERATIVE DIAGNOSIS:
- Posterior root avulsion of the medial meniscus Left knee.
- Grade 3-4 Patellofemoral arthritis Left Knee.
- Grade 2-3 Arthritis of the medial femoral condyle Left knee.
Surgery Performed:
- Left knee Arthroscopic Medial Meniscus root repair with transosseous tunnel and endobutton.
- Chondroplasty of Patellofemoral joint left knee.
- Chondroplasty of Medial Femoral Condyle
DESCRIPTION OF PROCEDURE: The patient was taken to the operating room where general anesthesia was induced. She was placed on a well-padded operating table. IV antibiotics were given. The left lower extremity was prepped and draped aseptically in the usual fashion. A low tourniquet was applied. The tourniquet was inflated. A timeout was called.
A lateral entry portal was made and the scope was entered. A tear of the posterior horn of the medial meniscus was found. A medial entry portal was made. The probe was inserted and the tear was re-examined. It was found to have a root avulsion of the posterior horn of the medial meniscus.

Intraoperative Arthroscopic images.
There was Grade 3-4 patellofemoral arthritis as well as Grade 2-3 medial femoral condyle arthritis. A decision was made to do the root repair. Chondroplasty of patellofemoral arthritis which was grade 2 to grade 3 and medial femoral condyle was performed.
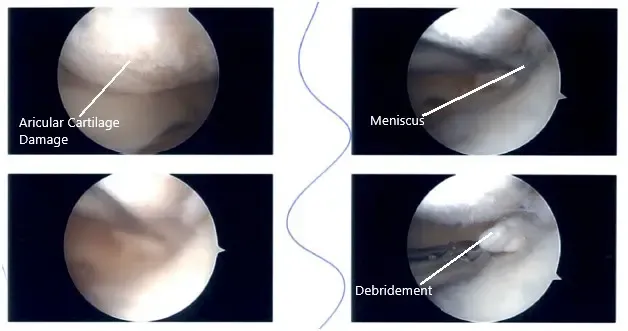
Intraoperative Arthroscopic images.
FiberWire #2 suture was passed using scorpion through the root after preparation. Curette was used to prepare the bed by removing the articular cartilage as well as the bone. ACL zig was used to locate the site for the insertion of the root. Guiding through the ACL zig, an incision was given laterally onto the shin and the guide was inserted. A 2.5-mm drill bit was used to drill to the site of insertion.
Finding it satisfactory, a suture retriever was inserted. The sutures were passed through the suture retriever and retrieved out of the lateral shin of the tibia. Finding it in a satisfactory position on tightening, the sutures were tied over an EndoButton. The loose body reported on MRI was embedded deep and loose so it was decided to leave it as such. Final pictures were taken. The knee was irrigated thoroughly.
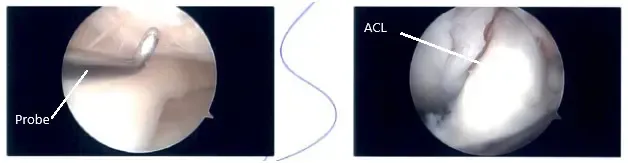
Intraoperative Arthroscopic images.
The closure was performed using #4-0 nylon. Then 20 cc of Naropin was injected into the knee. The dressing was done using 4 x 4, ABD, Webril, Ace wrap, and a knee immobilizer was applied. The patient was extubated and moved to the recovery in stable condition.
The patient was informed to wear the knee immobilizer and to be weight-bearing as tolerated with the knee in extension. He can remove the immobilizer and bend the knees up to 90 degrees without weight-bearing. He is advised to use the walker for ambulation.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
