A revision total knee replacement is surgery to fix a knee replacement that has worn out, loosened, “failed”, or run into a complication like infection, fracture, or instability.
The surgeon removes the old implant and revises it into a new replacement. It is more complex than the first replacement, takes longer, and often needs specialized implants and careful planning. The goal is the same as the original: less pain and better movement so you can get back to daily life.
Why knee replacements fail
A knee implant often lasts 20 years or more, but it can fail sooner, especially in younger, very active people or those with certain health conditions. Failure of a replacement usually comes from one or more of these:
- Infection: the metal and plastic parts can give bacteria a surface to grow on that the immune system cannot reach. This is one of the most common causes of early failure.
- Aseptic loosening: the most common late cause, where tiny movement at the joint between bone, cement, and metal gradually loosens the parts.
- Osteolysis: wear particles from the plastic insert trigger the immune system, which in clearing them also erodes the surrounding bone and loosens the implant.
- Fractures of the bone around the implant, where the repair depends on the location of the break.
- Instability from implants that were not fixed or positioned well, or from loose ligaments on the inner or outer side of the knee.
- Metal hypersensitivity, which may need a switch to more body-friendly implants.
- Scar tissue under the quadriceps tendon, which can cause a clunk as the knee straightens.
Who is more likely to need a revision
Patient factors matter. Younger, more active people tend to wear out an implant sooner than older, less active people, and those who are overweight or have had previous knee surgery have a higher risk of infection.
Symptoms of a failing knee replacement
Warning signs include pain, swelling, stiffness, warmth, redness, fever, a limp, or a feeling of instability.
Pain when putting weight on the knee is common with mechanical loosening, while fever and feeling unwell point more toward infection. Some people notice a clunk or trouble fully bending or straightening the knee.
How it is diagnosed
Diagnosis starts with a detailed history and exam, checking the knee’s movement, strength, and stability.
X-rays show loosening, alignment, and bone loss. A CT scan helps assess where the components sit, an MRI can show bone damage, and a bone scan can pick up infection or loosening.
If infection is a concern, fluid is drawn from the joint and blood tests are done to look for it.
Other problems can mimic a failing implant, including tendon irritation, bursitis, a pinched spinal nerve, and hip arthritis, so the workup also confirms the trouble is coming from the knee itself.
Types of revision surgery
Revisions are described by what failed (loosening, infection, instability, fracture, or worn parts) and by how much is replaced. A partial revision swaps just one part, while a full revision replaces several. How much bone has been lost and how stable the ligaments are help decide which implants are used.
When revision surgery is needed
Mild symptoms can sometimes be managed for a time with medication, therapy, or bracing, but most true implant failures need surgery to fix the underlying problem.
The revision procedure
The surgery is planned in advance based on the condition of the implant and the bone, and it usually takes longer than the first replacement because the old parts must be removed carefully and the exposure is more involved.
When infection is the cause, treatment depends on how severe it is and how recently it started. A recent infection may be treated by washing out the joint and exchanging just the plastic parts, or by removing and replacing the implant in a single operation.
A more established infection is often handled in two stages: the first surgery removes the implant, thoroughly cleans the joint, and places a temporary antibiotic-loaded cement spacer. After a few weeks of intravenous antibiotics, and a repeat joint fluid test to confirm the infection is gone, the new implant is put in at a second surgery.
A fracture around the implant may need a special long-stem implant depending on where the break is, and a worn-out plastic insert may be replaced on its own, sometimes with bone grafts or cones to make up for bone lost during removal.
")
Revision knee replacement implant (semi – constrained with a long stem).
Special implants for bone loss and instability
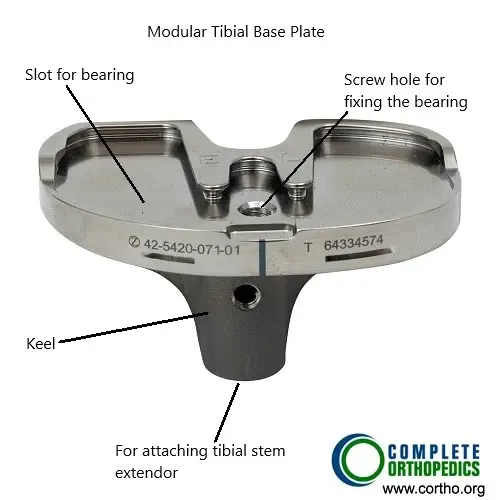
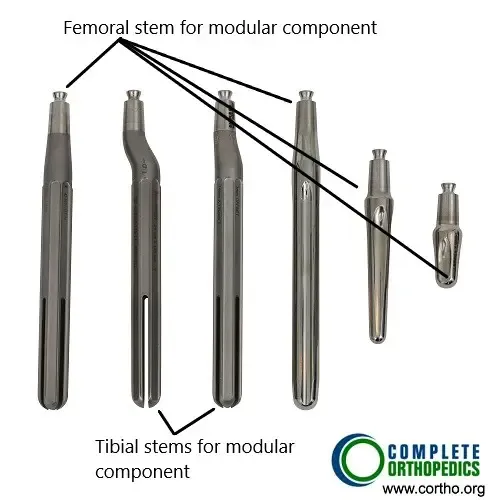
Revision surgery often uses parts the original did not. Modular components let the surgeon make adjustments during surgery and attach stems or bone augments to handle missing bone. Constrained plastic inserts use a tall, wide central post to add side-to-side and rotational stability, paired with stemmed components that spread out the extra stress.
To rebuild areas of bone loss, surgeons may use metal cones and metaphyseal sleeves, plus a bone graft taken either from elsewhere in your own body or from a bone bank. Longer stems and more constrained implants improve fixation and reduce instability.

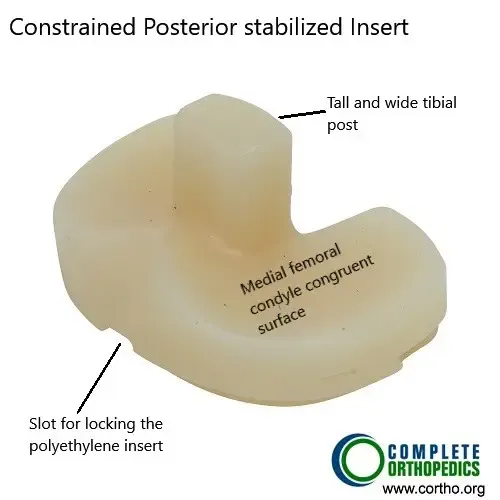
Constrained posterior stabilized polyethylene insert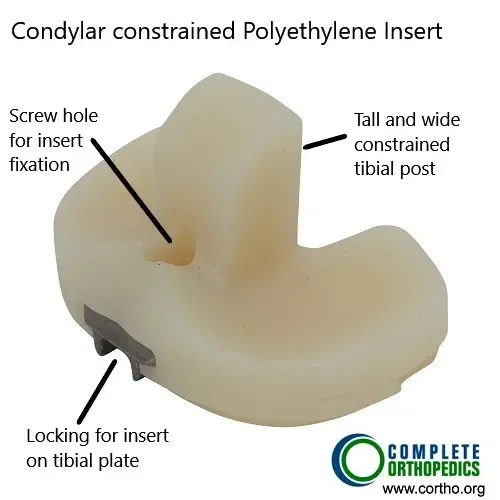
Revision knee replacement recovery
Most people stay in the hospital for several days. Pain medicine and early physical therapy get the knee moving, and therapy continues for several months.
Simple home adjustments like handrails and a walker help with safety. Follow-up visits check that the implant is working well. Full recovery can take up to a year, and staying active and keeping a healthy weight both support the result.
Risks of revision knee replacement
Revision surgery carries higher risks than a first-time knee replacement. They include infection, blood clots, fractures, nerve or blood-vessel injury, stiffness, and instability. The early weeks carry the highest chance of infection or clots, while the longer-term risks include loosening, wear, and the possibility of needing another revision down the road.
Long-term outlook
Most revision knee replacements are done without complications, and many people gain real improvement in comfort and mobility.
Some have mild ongoing pain that can be managed with medication and physical therapy. How well it goes depends on your overall health and other medical conditions, the reason for the revision (an infection, for instance, is more involved than simple wear), and the experience of the surgical team.
Implant materials and surgical techniques continue to improve, and outcomes along with them.
Insurance & Cost
Revision Total Knee Replacement Surgery at Complete Orthopedics is covered by Medicare and most major insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), as well as most workers’ compensation and no-fault insurance plans. Your out-of-pocket cost depends on your specific plan, deductible, and the medical necessity criteria that apply to your case.
How Medicare Covers Revision Total Knee Replacement Implants
If you have Medicare, your healthcare provider may bill for CPT Code 27487. This is a surgical procedure where a worn or failed knee implant is removed and replaced with new artificial components, both on the thigh bone (femur) and shin bone (tibia).
What is our out-of-pocket cost?
Estimated Out-of-Pocket Cost for Revision Total Knee Replacement Implants (27487): $354.05
Medicare approves about $1,770.25 for this procedure and pays 80% of it ($1,416.20). The remaining 20% is the patient’s responsibility.
“For example, hypothetical patient, Maria, had a knee replacement 15 years ago that had worn out and become loose. Her surgeon removed the old implant and replaced it with new femoral and tibial components (27487). Thanks to Medicare, her total out-of-pocket cost was about $354.05. Her secondary insurance then covered it completely!”
Call our billing team at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs. For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
Do you have more questions?
How long does a revision knee surgery take?
The duration of revision knee surgery can vary, but it generally takes between 2 to 3 hours, depending on the complexity of the case.
Can revision knee surgery be done on an outpatient basis?
Revision knee surgery is generally more complex and is usually performed in a hospital setting with an expected stay of 1-3 days, unlike some primary knee replacements that can sometimes be done on an outpatient basis.
Will I need physical therapy after revision knee surgery?
Yes, physical therapy is crucial for recovery after revision knee surgery. It helps to restore strength, flexibility, and function to the knee.
How painful is revision knee surgery compared to the initial knee replacement?
Pain levels can vary, but many patients report that the pain after revision surgery is similar to or slightly more than the initial knee replacement due to the complexity of the procedure.
What are the success rates for revision knee surgery?
Success rates for revision knee surgery can vary but are generally around 85% to 90%, depending on the reason for the revision and the patient’s overall health.
How long will the new implant last after revision surgery?
While there is no guarantee, a well-performed revision knee surgery with proper implants can last 10-25 years, similar to primary knee replacements.
What lifestyle changes should I make after revision knee surgery?
Post-surgery, it’s important to maintain a healthy weight, stay active with low-impact exercises, and avoid activities that put excessive stress on the knee.
What should I do if I experience complications after revision knee surgery?
Contact your surgeon immediately if you experience signs of infection (fever, redness, or drainage), severe pain, or if you have difficulty moving the knee.
How can I prepare my home for recovery after revision knee surgery?
Preparing your home for recovery includes installing handrails, keeping essential items within reach, and possibly arranging for a raised toilet seat or shower chair.
Will I need help at home after revision knee surgery?
Yes, it’s advisable to have someone assist you at home during the initial recovery period to help with daily activities and transportation to follow-up appointments.
How often will I need to see my surgeon after revision knee surgery?
Follow-up visits typically occur at two weeks, six weeks, three months, six months, and then annually to monitor the implant and overall recovery.
Can revision knee surgery address alignment issues from my first knee replacement?
Yes, one of the goals of revision surgery is to correct any alignment issues that may have occurred with the initial knee replacement.
What dietary changes should I make to aid my recovery after revision knee surgery?
A balanced diet rich in protein, vitamins, and minerals can help in healing. Staying hydrated and possibly taking supplements as recommended by your doctor can also aid recovery.
Is it normal to feel numbness around the incision site after revision knee surgery?
Yes, some numbness around the incision site is normal due to nerve disruption during surgery, and it may persist for several months.
Are there any special exercises I should do before revision knee surgery?
Preoperative exercises focusing on strengthening the quadriceps, hamstrings, and maintaining range of motion can help improve postoperative recovery.
How can I prevent infections after revision knee surgery?
Preventing infections includes proper wound care, following your surgeon’s instructions for hygiene, and possibly taking antibiotics as prescribed.
What type of support will I need for mobility after revision knee surgery?
Initially, you will likely need crutches or a walker. As you progress in your recovery, you may transition to a cane before becoming fully independent.
How does bone quality affect the success of revision knee surgery?
Good bone quality is crucial for the success of the surgery as it affects the stability and longevity of the new implant. Bone grafts may be used if there is significant bone loss.
Can I drive after revision knee surgery?
You can usually start driving again once you have regained sufficient strength and mobility in your knee and are no longer taking narcotic pain medications, typically 4-6 weeks post-surgery. Always get your surgeon’s approval before resuming driving.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.

