The patient had been seen by me in the office multiple times with complaints of pain in the lower back radiating to the left lower extremity. The patient has a history of discectomy in the past in 2011.
They had been treated conservatively in the form of physical therapy as well as epidural injections which gave short-term relief to their back pain as well as leg symptoms.
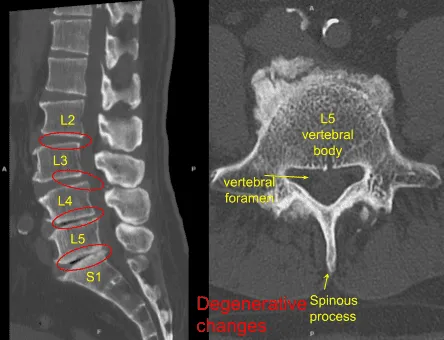
They got an MRI done which showed degenerative changes from L2 to S1 with retrolisthesis in L2-L3, grade 1 anterolisthesis at L3-L4, vacuum phenomena at L4-5 and L5-S1 with loss of disc space at L4-L5 and L5-S1.
We discussed treatment options and having failed all conservative management, the patient agreed for operative management in the form of L2 to S1 lumbar decompression and fusion.
We discussed risks and complications including infection, bleeding, injury to adjacent nerves and vessels, failure of surgery and failure of implants, need for repeat surgery, CSF leak and possible need for repeat surgery, no resolution of pain, worsening of symptoms among others.
We discussed systemic complications including blood clots, cardiac, pulmonary, neurological complications among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. Neuromonitoring was established. Foley catheter was passed. The patient was put prone on a four-post Jackson table. All the bony prominences were well padded. The lower leg was prepped and draped aseptically in the usual fashion. A time-out was called. Preop antibiotic was given.
An incision was given along the same incision. With sharp dissection, the spinal process could be reached. With Bovie and blunt dissection, the spinous processes of L2 to S1 were exposed bilaterally onto the facet joint with exposure of the TPs on L2, L3, L4, L5 and sacral ala on both sides. Allis clamp was put on the right L2 and L5 and localization was done with the use of x-ray and found to be in the correct position.
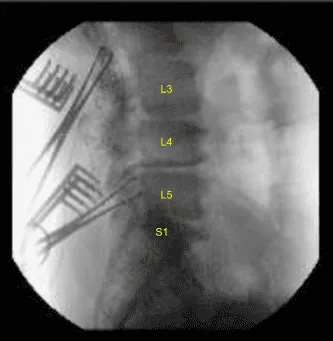
The navigation was brought in and CT scan was performed. After the navigation was verified, pedicle screws were put on both sides of L2 to S1 sequentially under navigational guidance after using gear shift, tapped and checked every time with a ball tip probe.
Acceptable positions were achieved on all the levels. The screwdriver tip was broken on the right S1 screw, but was left in situ because it was difficult to get it out and would have led to loosening.
Posterior osteotomies of the lamina and the inferior facet as well as superior facet were done over the right L5-S1, left L4-5, right L2-3 as well as bilateral L3-4. Complete laminectomy was done over L3-4 along with and bilateral foraminotomy of L3-4 was performed followed by laminotomy and foraminotomy of right L5-S1, left L4-5 and right L2-3.
Annulotomy and thorough discectomy was performed on L2-3 from the right, L3-4 from the left, L4-5 from the left and L5-S1 sequentially with the use of paddles and curettes.
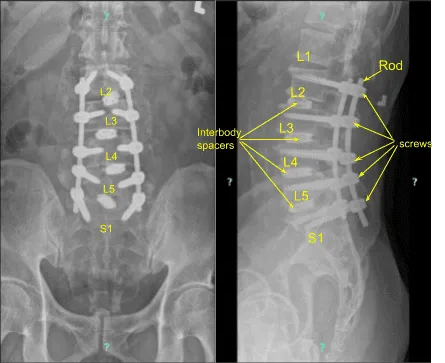
Thorough discectomy was performed and disc was removed with a pituitary. Interdiscal space were irrigated and drained and packed with local autograft bone and Expandable cages packed with bone, were inserted one disc space at a time and expanded in acceptable position under fluoroscopic guidance.
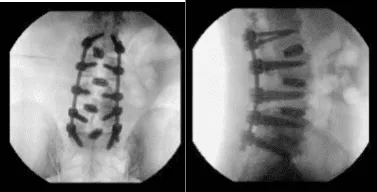
The rods were put onto the pedicle screws and tightened in place with set screws and final tightening with the use of torque lifting screwdriver. Final pictures were taken and found to be in acceptable position.
The wound was thoroughly irrigated and drained. Local auto Bone graft mixed with actifuse was laid into the gutters in the right and left side between the L2 to S1. Hemostasis was achieved. Closure was done by the Plastic Surgery Team and it will be dictated separately.
Neuromonitoring was intact throughout the procedure. Final CT scan was also performed to check the position of cages and the screws and were found to be in acceptable position. After the closure, the patient was extubated and moved to recovery in a stable condition.
The patient followed up 14 days after their surgery. They continued to follow up 4, 6, and 8 weeks after the surgery and showed signs of gradual improvement.
In their last office visit the patient stated they were doing really well after the surgery. The patient is doing a lot better with their back pain. They have resumed regular activities such as playing tennis.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
