The patient presented to the neurosurgery clinic with signs and symptoms of lumbar spondylolisthesis, stenosis and spondylotic radiculopathy having failed nonsurgical treatment. They previously underwent posterior cervical laminectomy and fusion.
Surgery was recommended to decompress and stabilize her lumbar spine. The risks, benefits, alternatives, and potential complications were explained to her. All of their questions were answered until no further issues were raised and she provided written informed consent which was placed in the chart.
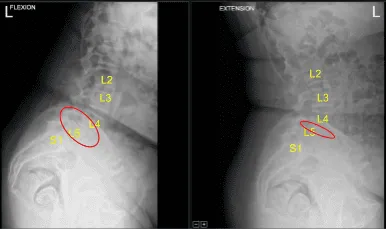
Anterolisthesis of L4 on L5 with dynamic instability during flexion and extension
The patient was brought to the operating room. Their identity was verified. General anesthesia was induced. They were intubated by the Anesthesia Service. Respiratory and cardiac monitoring leads were placed. Neuromonitoring leads for somatosensory evoked potentials and EMG were placed. They received preoperative prophylactic IV antibiotics and IV tranexamic acid. Surgical timeout was performed. They were positioned prone on a Jackson Relton-Hall frame.
All pressure points were padded. Lumbar area was cleaned with chlorhexidine and sterilized with a DuraPrep solution. 22-gauge spinal needle and fluoroscopy were used to localize the L4-5 level. Skin was sterilized with DuraPrep solution. Sterile drapes were placed in the usual manner. An intraoperative stereotactic image-guided frameless neuronavigation array was placed on the left superior posterior iliac crest.
After infiltrating with local anesthesia, #15 blade stab incisions were made and Schanz pins were placed into the iliac crest and neuronavigation array was affixed. The patient was draped sterilely. Intraoperative CT scan was performed.
Data was transferred to the neuronavigation computer and accuracy was verified. Stereotactic image-guided neuronavigation techniques were used to identify starting points and trajectories and demarcate bilateral approximately 2.5 cm incisions. Skin was infiltrated with 1% lidocaine and epinephrine.
We began on the left side. The skin was opened with a #15 blade scalpel. Hemostasis was obtained with Bovie and the fascia was sharply divided with the Bovie. K-wireless self-drilling, self-tapping 6.0 x 45 mm titanium pedicle screws were placed using neuronavigation in the left L4 and L5 pedicles without difficulty.
Next, attention was turned to the right side. Skin was infiltrated with local anesthetic. Skin was opened with #15 blade scalpel. Hemostasis was obtained with Bovie, monopolar and electrocautery. The fascia was sharply divided with the Bovie.
Navigated Jamshidi needles were gently tamped into the L4 and L5 pedicles with a mallet. The stylets were removed, and K-wires were placed after which the Jamshidi needles were removed, and the K-wires were snapped down to the drapes with hemostats.
C-arm unit, which was draped sterilely, was brought into the field and used with tubular sequential dilators to dock a 7 cm x 22 mm diameter tubular retractor on the right L4-5 facet joints. The tubular retractor was affixed rigidly to the bed frame.
The operative microscope was balanced, draped sterilely, and brought into the field and the remainder of the procedure was performed using microsurgical instruments and techniques for micro dissection for the facetectomy and decompression. Bovie, monopolar and pituitary rongeurs were used to resect soft tissue overlying the facet joints.
An electric high-speed drill under sterile saline irrigation was used to perform the facetectomy. The annulus was exposed. The ligamentum flavum was retracted with Kerrison rongeurs. Bone bleeding was controlled with bone wax and Surgiflo hemostatic matrix. Annulotomy was performed with retractable bayoneted #15 blade scalpel. Discectomy was performed with sequential paddle shavers as well as straight and angled pituitary rongeurs.
The interspace was irrigated clear. The endplates at L4-5 were prepped for the arthrodesis with angled curettes and rasps. Morselized autograft collected with the Hensler during the decompression was mixed with ViviGenallograft which was then placed into the L4-5 interspace with funnel and tamp.
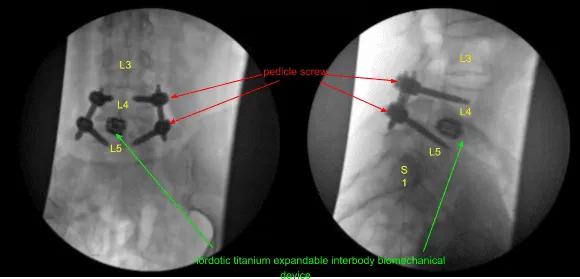
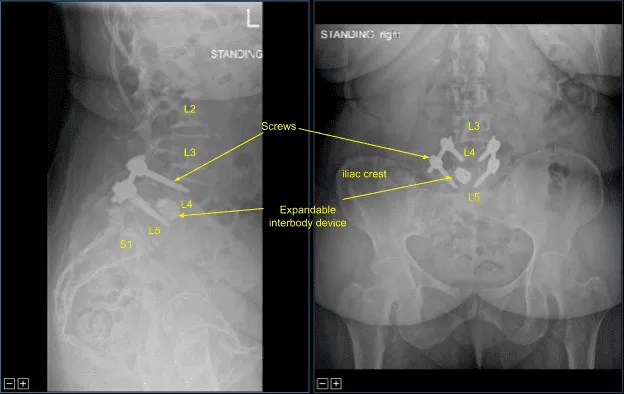
A 22 mm long lordotic titanium expandable interbody biomechanical device was placed through an inserter into the interspace under AP and lateral fluoroscopic guidance and expanded to the proper fit and tightness. The inserter was removed. The tubular retractor was then withdrawn under microscopic visualization to confirm hemostasis with the bipolar electrocautery.
Next, cannulated self-tapping 6.0 x 45 mm titanium pedicle screws were placed over the K-wires at L4 and L5 on the right side under fluoroscopic guidance. K-wires were removed. The screws were advanced until proper tightness was achieved and depth. Neuromonitoring signals were stable throughout. The patient was redraped.
A second intraoperative CT scan was performed showing correct positioning of all of the implanted hardware and instrumentation. Next, calipers were used to determine the length of precut-precontoured titanium rods which were placed across the bilateral L4-5 non segmental pedicle screw instrumentation tulip heads and secured with locking caps.
These were first tightened at L5 bilaterally and then at L4 to achieve reduction of the spondylolisthesis. Approximately 50% reduction was achieved. The locking caps were then final tightened with a torque and anti torque device. The pedicle screw extender tabs were then removed. The wounds were irrigated copiously. Hemostasis was confirmed again.
Vancomycin powder was applied. Schanz pins and neuronavigation array were removed. The fascia bilaterally was closed in watertight fashion with 0 Vicryl sutures. Exparel long- acting local anesthetic was infused into the soft tissues.
The subdermal layers were closed with 2-0 Vicryl sutures and the skin closure was achieved with running 4-0 Monocryl subcuticular stitches. The incisions were then cleaned and dried sterilely and dressed with Prineo Dermabond dressing.
The patient was then turned supine on the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient followed up two weeks after the surgery and then continued following up in our office 4, 6, 8, 12, 24 weeks with sequential X rays. In their last office visit the patient stated they were able to do their usual activities and that physical therapy was going well.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
