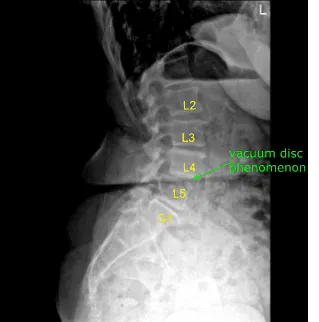
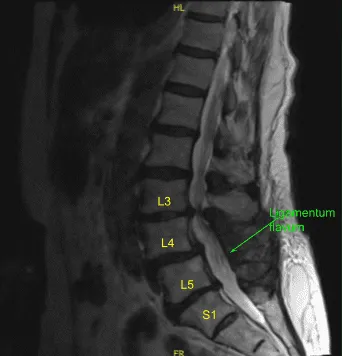
A patient presented to a neurosurgery clinic with signs and symptoms of lumbar stenosis with neurogenic claudication and a right-sided foot drop. Imaging showed severe stenosis at L4-5 centrally and L5-S1 on the left. Surgery was recommended to decompress her lumbar spine.
The risks, benefits, alternatives and potential complications were explained to her. All of her questions were answered until no further issues were raised and they provided written informed consent which was placed in the chart.
The patient was brought to the operating room. Their identity was verified. General anesthesia was induced, and they were intubated by the Anesthesia Service. Respiratory and cardiac monitoring leads were placed.
Neuromonitoring leads for somatosensory evoked potentials and EMG were placed and baseline signals were obtained. They received prophylactic IV antibiotics due to penicillin allergy.
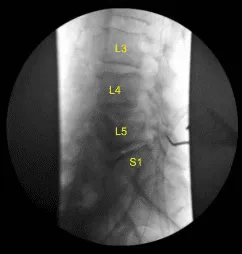
They were positioned prone on a Wilson frame. All Pressure points were carefully padded. Lumbar area was cleaned with chlorhexidine. A 22-gauge spinal needle and fluoroscopy was used to localize the L4-5 level.
A midline incision was demarcated. Skin was sterilized with a DuraPrep solution. Sterile drapes were placed in the usual manner. 1% lidocaine with epinephrine was infused. Skin was opened with a#10 blade scalpel.
Hemostasis was obtained with bipolar electrocautery. Bovie monopolar was used to carry the incision down through subcutaneous tissues and sharply divided the fascia. Cobb elevators and Bovie were used to expose the L4 lamina bilaterally and L5 on the left.
McCullochself-retaining retractor system was placed. A Woodson elevator was placed into the L4 lamina. The C-arm unit, which was draped sterilely, was brought into the field and used to confirm the level. The L4 spinous process was respected with a Leksell rongeur.
Laminectomy was performed with electric high-speed drill under continuous sterile irrigation exposing hypertrophied ligamentum flavum which was resected in piecemeal fashion with Kerrisonrongeurs, carefully protecting the dura with Woodson elevator, and removed with #4 Penfield.
Lateral recesses were decompressed bilaterally.Bilateral exiting L4 nerve roots were completely neurolyzed withMetzenbaum-Penfield technique and confirmed with nerve hooks and Woodsonelevator.
Next, McCulloch retractor was moved caudally to L5 on the left.Left L5 laminotomy was performed with Kerrison rongeurs and electric high-speed drill. Dura was carefully protected. No durotomy was identified. Epidural bleeding was controlled with bipolar electrocautery and Surgiflo hemostatic matrix.
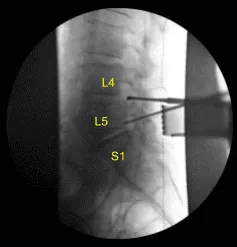
We took a final x-ray confirming decompression of the foramina with a Woodson and a Penfield #4 in the L4-5 and L5-S1 foramina on the left side. The wound was irrigated copiously.Hemostasis was confirmed.
A medium size Hemovac drain was tunneled in a subfascial manner and secured to the skin with a 3-0 nylon suture. Thefascia was closed in watertight manner with interrupted 0 Vicryl sutures. Exparel long acting local anesthetic was infused into the soft tissues. The Subdermal layer was closed with 2-0 Vicryl sutures.
The skin was reapproximated with a running subcuticular 3-0 Monocryl. The incision was cleaned, dried and dressed sterilely with Prineo Dermabond dressing. Hemovac canister was applied to suction.
The patient was then turned supine on the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts and instrument counts were correct. The patient tolerated the procedure well.
The patient initially followed up in one week after the surgery and then continued following up in our office 4, 6, 8, 12 weeks. Patient is doing well.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
