The patient presented to our clinic with signs and symptoms of lumbar stenosis. Having failed nonsurgical treatment, surgery was recommended to decompress the lumbar spine. The risks, benefits, alternatives, and potential complications of the surgery were explained to him.
All of their questions were answered, and they provided written informed consent which was placed in the chart. Their significant other was present for the informed consent and their questions were answered as well.
The patient was brought to the operating room. Their identity was verified. Surgical timeout was performed. General anesthesia was induced. They were intubated by the Anesthesia Service. Respiratory and cardiac monitoring leads were placed.
Neuromonitoring leads for somatosensory evoked potentials and EMG were placed and baseline signals were obtained. They received preoperative prophylactic IV antibiotics. They were positioned prone on a Wilson frame. All pressure points were padded.
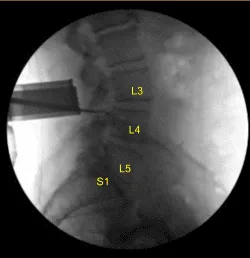
Lumbar area was prepped with electric hair clippers and cleaned with chlorhexidine. Spinal needle and fluoroscopy were used to localize the L3-4 level. Skin was sterilized with a DuraPrep solution. Sterile drapes were placed in the usual manner. C-arm unit was draped sterilely for localization.
Midline incision was performed with #15 blade scalpel after infiltrating with 1% lidocaine and epinephrine. Hemostasis was obtained with bipolar electrocautery. Bovie and monopolar was used to carry the incision down through the subcutaneous tissues and sharply divided the fascia and performed subperiosteal dissection of the L3 and cephalad L4 lamina. A Woodson elevator was placed under the L3 lamina.
C-arm unit was used to confirm the level. Bovie and Leksell rongeurs were used to resect the spinous process. An electric high-speed drill under continuous sterile irrigation was used to perform L3 laminectomy and partial L4 laminectomy.
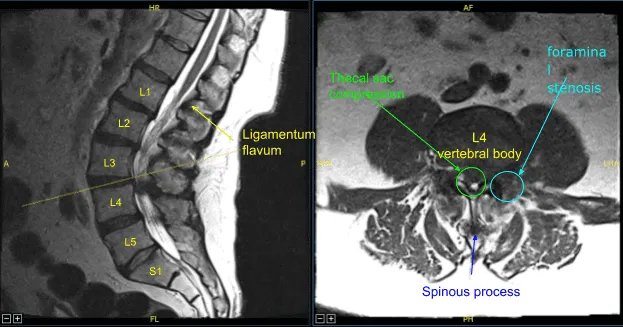
Ligamentum flavum was exposed and was noted to be significantly hypertrophied. Extensive arthritic changes and osteophytes were noted in this part of the spine. Kerrison rongeurs were used to resect the ligamentum flavum exposing the dura.
Decompression was continued laterally until the thecal sac was fully decompressed. While decompressing the lateral recess with Kerrison rongeurs and exploring the lateral recess with Penfield instruments, a very small amount of clear fluid was seen. It was not determined if this was secondary to synovial cyst seen on preoperative MRI or a cerebrospinal fluid leak.
Thecal sac turgor was maintained. The dura was inspected, and in the anterolateral aspect, a small possible arachnoid bleb was seen. Even though no spinal fluid was seen egressing from this, a 4-0 Nurolon stitch was placed as well as a piece of fat and at the end of the procedure DuraSeal fibrin glue.
Valsalva maneuvers were performed and again this produced no cerebrospinal fluid Leak. Hemostasis was obtained throughout the procedure with Surgiflo hemostatic matrix, bone wax and bipolar. Bilateral L3 nerve roots were fully neurolyzed with Metzenbaum-Penfield technique.
Decompression confirmed with Woodson elevators. The wound was irrigated copiously, and then once decompression was deemed adequate, closure was performed with watertight reapproximation of the fascia with 0 Vicryl sutures.
Exparel long- acting local anesthetic was infused into soft tissues. The subdermal layer was closed with 2-0 Vicryl sutures and the skin was reapproximated with a running 3-0 nylon and then cleaned and dried sterilely, and dressed with Xeroform, Telfa, and Tegaderm.
The patient was then turned supine on the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient followed up two weeks after the surgery in our outpatient clinic. The patient stated they had experienced improvements with their back pain and showed little to no signs of lumbar stenosis.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
