The patient was complaining of pain in both lower extremities. They had a history of L3 to S1 fusion done by another physician. Imaging studies showed good fusion mass from L3 to S1 but compression over L2-L3 segment with bilateral neural foraminal compression of L3 along with bony island formation over L3-L4 region with foraminal compression.
We discussed treatment options and opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, dural leak and possible repair, failure of surgery, need for rehabilitation, need for repeat surgery, need for fusion in future, systemic complications including blood clots, cardiac, pulmonary, neurological complications including death. The patient understood and signed an informed consent.
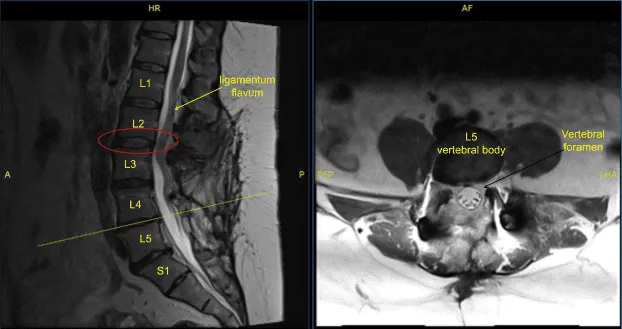
Disc bulge, facet osteoarthritis, buckling of ligamentum flavum
The patient was taken to the operating room where they were intubated and performed general anesthesia. A Foley catheter was inserted. The patient was placed prone on the Jackson table. All bony prominences were well padded. The lower back was prepped and draped aseptically in the usual fashion with the use of alcohol followed by DuraPrep. A timeout was called. Pre operative antibiotics and TXA were given.
The posterior midline incision was already present from the previous surgery. Exposure was planned along the superior part of the incision and extended proximally to expose the L2-L3 level. The skin incision was given. Dissection was carried deep along the subcutaneous fascia followed by deep fascia. Spinous process of L2 was reached. Dissection was carried down on either side of the spinous process and lamina of L2 onto the facet joint.
The dissection was carried distally along the scar tissue and the scar was excised from over the L3 laminectomy defect. Further laminectomy was done of L2 with the use of rongeur followed by Kerrison punch. A further laminectomy of L2 was performed and decompression of the L2 nerve roots on either side was performed with the use of Kerrison punch and checked with the use of Woodson.
Curettes were used to delineate the L3 nerve root and the foramen on either side followed by decompression of the L3 nerve roots with the use of Kerrison punch. Further distal exposure showed the bone formation along the posterior elements of L3 and L4.
The revision of laminectomy of L3 and L4 was performed with the use of bur, Kerrison punches. Decompression of bilateral L3 and bilateral L4 nerve roots were performed with the use of curettes followed by Kerrison punch and the decompression was checked with the use of Woodson. A thorough decompression of bilateral L2, L3 and L4 was achieved after laminectomy of L2 and revision laminectomy of L3 and L4.
Final x-rays were again taken and saved. Hemostasis was thoroughly achieved. Wound was thoroughly irrigated and drained. Closure was done with the help of a plastic surgeon considering the complexity of the skin closure.
Patient did well in the post op period and was discharged after 2 days of stay in the hospital. She was followed in the office and did well with full resolution of the pain. She started physical therapy at 4 weeks and went to make a complete recovery in 3 months.
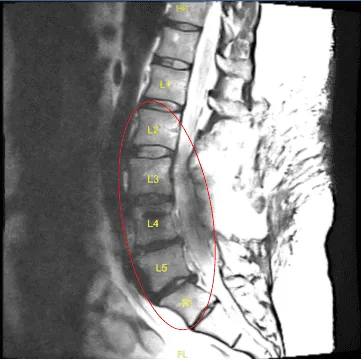
Status post posterior decompression the spinal canal from L2 through S1
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
