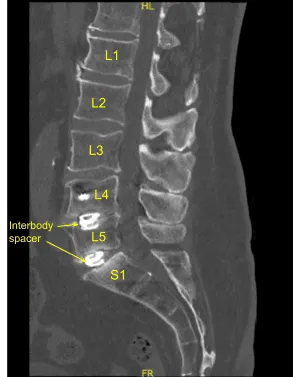
This patient previously underwent L4 to S1 minimally invasive transforaminal lumbar interbody fusion. They did well and recovered, however subsequently developed recurrence of their low back pain, had various injections and nonsurgical treatments including a sacroiliac joint fusion.
However, their back pain only worsened. Imaging showed loosening of bilateral pedicle screws and signs of pseudarthrosis. Surgery was recommended to stabilize the lumbar spine. The risks, benefits, alternatives and potential complications of the surgery were explained to them.
All of their questions were answered until no further issues were raised and they provided written informed consent which was placed in the chart.
The patient was brought to the operating room. Their identity was verified. Surgical timeout was performed. General anesthesia was induced. They were intubated by the Anesthesia Service. Respiratory and cardiac monitoring leads were placed.
Neuromonitoring leads for somatosensory evoked potentials and EMG were Placed. They received preoperative prophylactic IV antibiotics. They also received IV tranexamic acid. They were positioned prone on a Jackson Relton-Hall frame with all pressure points carefully padded.
Lumbar area was prepped with an electric hair clipper, cleaned with chlorhexidine and sterilized with a DuraPrep solution. A midline incision was demarcated. Sterile drapes were placed in the usual manner. 2% lidocaine with epinephrine was infused along the skin line.
The skin was opened with a #10 blade Scalpel. Hemostasis was obtained with bipolar electrocautery. Bovie monopolar and Cobb elevator were used to perform subperiosteal dissection exposing posterior elements of the spine from L4 to sacrum including previous spinal hardware pedicle screw-rod construction from L4 to S1. Self-retaining retractors were placed. Locking caps were removed x6 on both sides. The rods were removed. The fusion was explored and found to be inadequate.
Loosening of bilateral sacral screws was confirmed and they were removed. We placed the neuronavigation array and fixed it rigidly to the posterior superior iliac crest with two Schanz pins.
The patient was draped sterilely. CT scan was obtained, and data was transferred to the neuronavigation computer. Neuronavigation techniques were used to reposition and replace bilateral sacral screws which were upsized both in diameter and length until tight.
We also replaced the left L4 and L5 pedicle screws similarly with a new track screw aided by decorticating with electric high-speed drill, cannulating with navigated pedicle finder, palpating for breaches, measuring the depth, under tapping by 1 mm and placing the pedicle screws without difficulty.
Additional CT scans were performed showing correct positioning of all the pedicle screw hardware. Neuromonitoring signals were stable. Next, we decorticated bilateral transverse processes and facet joints including sacral ala from L4 to S1 bilaterally with electric high-speed drill for the arthrodesis. The wound was irrigated copiously.
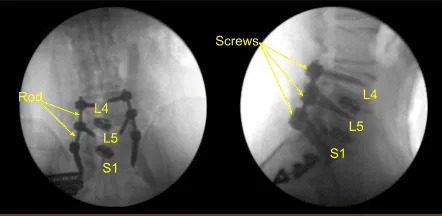
Precut-precontoured titanium rods were selected, contoured further and placed across the tulips from L4 to S1 bilaterally and secured with locking caps which were all final tightened with a torque and anti torque device. AP and lateral fluoroscopy was used to confirm appropriate sizing and positioning of the rods.
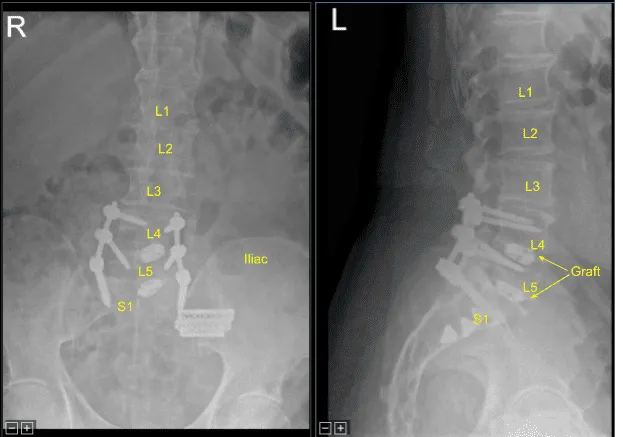
Next, morselized autograft resected from spinous processes of L4 and L5, which was morselized in the bone mill, was mixed with demineralized bone matrix allograft putty as well as bone morphogenic protein. We aspirated iliac crest bone marrow through a separate incision created for the Schanz pin with a bone marrow aspirator. This was mixed as well.
These were packed in lateral gutters and across the facet joints after decortication from L4 to S1 for arthrodesis.The wound was irrigated clear. Hemostasis was obtained with bipolar electrocautery and bone wax.
Vancomycin powder was applied liberally.Medium size Hemovac drain was tunneled in a subfascial manner and secured to the skin with 3-0 nylon suture.Interrupted 0 Vicryl sutures were placed in a watertight fashion to reapproximate the fascia.
Exparel long-acting local anesthetic was infused into the muscles and then subdermal closure was accomplished with 2-0 Vicryl sutures and the skin was reapproximated with subcuticular 4-0 Monocryl, cleaned, dried sterilely and dressed with Prineo Dermabond dressing. Hemovac canister was applied to suction.
The patient was then turned supine on the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient initially followed up in 12 days after the surgery and then continued following up in our office 4, 6, 8, weeks after the surgery. The patient reported improvements with back pain. They were able to return to their daily activities.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on May 27, 2026.
