The patient had been in our office with complaints of lumbar spine pain and right anterior thigh sciatica for a few years. The Patient was diagnosed with Right L3 radiculopathy secondary to Right L2-3 disc herniation. The patient described the pain as burning, sharp, and stabbing.
The pain was constant and disturbed their sleep. The patient also reported the pain to be associated with numbness, tingling, radiating pain, gait problem. The pain was not associated with swelling, bruising, weakness, bowel or bladder abnormality, or limping, giving way, hand function difficulty.
He got multiple epidural injections in his back but the pain recurred. The problem was reported to be getting worse since it started. Standing after sitting makes the symptoms worse.
Rest, heat, ice, lying down, bending forwards makes the symptoms better. The patient has not undergone surgery in the past. The patient is right-handed. The physical examination supported the plan of a right L2-3 microscopic laminotomy, discectomy, foraminotomy.
Conservative treatment in the form of physical therapy and medications were tried. No improvement after conservative treatment, an MRI was performed. The MRI showed an extruded disc in the right L2-3. The patient tried an epidural injection which gave temporary relief. Finding no permanent relief, the patient opted for surgical management. The patient understood and signed an informed consent.
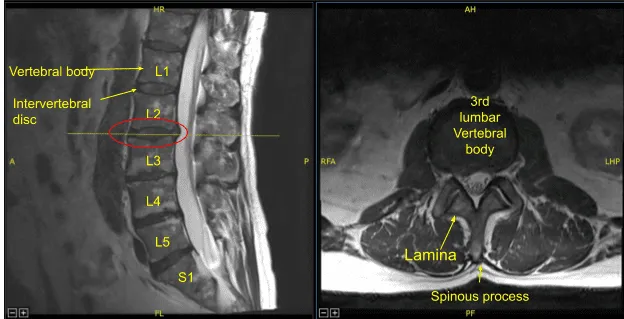
Diffuse disc bulge and superimposed right paracentral disc herniation
The patient was taken to the operating room and general anesthesia was induced. The patient was flipped on to their belly over a Jackson table with a Wilson frame. All bony prominences were well padded. Their elbows were well padded. The Lower the back was prepped aseptically and draped in the usual fashion. Preoperative antibiotics in the form of Ancef and vancomycin were given. Time-out was called.
A spinal needle was inserted into a presumed L2 vertebral body. C-arm was brought in and lateral views were taken and confirmed that the needle was at L2 pedicle. Skin incision was marked and the skin was incised using a #10 blade. Using Bovie a deep dissection was performed through the deep fascia and on the right side of the spinous process of L2 and L3.
The lamina of L2 and L3 were exposed up to the medial facet joint. Once hemostasis was achieved, the Woodson was inserted in the L2-3 disc space and C-arm was brought in for a lateral view. The level of L2-3 was re-confirmed and saved.
A Wilson retractor was used for lateral retraction; #2-0 nylon was used for retracting the tissue on the medial side. Operating microscope was brought in and was used for further surgical management. A high-speed burr was used to remove the inferior lamina of right L2. Using upgoing curette and Woodson, making a plane between the ligamentum flavum and lamina, Kerrison punch #2 and #3 were used to complete the laminectomy.
Further superior laminectomy of L3 was performed on the right side. The ligamentum flavum was excised to achieve central as well as lateral decompression. Woodson was used to break the adhesions over the Right L3 nerve roots.
Ball tip probe was also used to dissect the nerve root laterally. Love Nerve root retractor was used to retract the nerve roots medially and extruded disc fragments were exposed. Multiple fragments were removed using micro pituitary forceps. The disc space was sealed.
After removal of all loose fragments, irrigation of the surgical wound was performed. Far lateral decompression was checked and laminectomy and foraminotomy was completed. The right L3 nerve root was thoroughly decompressed. Hemostasis was achieved using bipolar cautery as well as Surgiflo.
After achieving satisfactory decompression, 4 cc of Surgiflo mixed with 40mg of Depo-Medrol was injected into the surgical area and the wound was closed in layers using 0 Vicryl followed by 2-0 Vicryl and 4-0 monocryl. Dressing was performed using 4×4 and Tegaderm. The patient was turned supine on the bed and extubated and moved to the recovery unit in stable condition. Post op neuro check was also performed and he was found to be intact.
Post-Op
The patient had relief in his thigh pain, though he had pain in his back at the surgical site. The patient followed up in one week and their pain was well resolved. They were able to do the usual activities of daily living. They were also able to do some yard work. The patient continued to follow up 4, 8, and 12 weeks after surgery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
