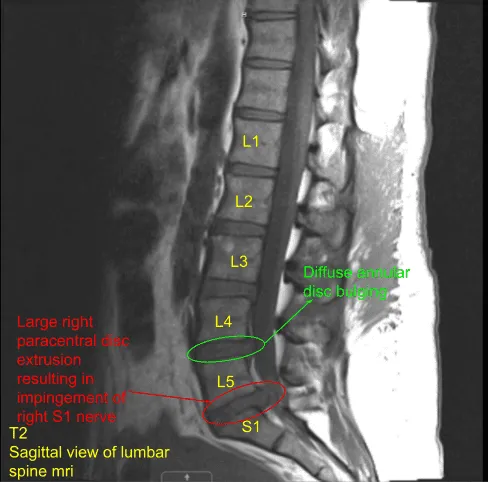
A patient presented with severe radicular pain on the right lower extremity, which was not relieved with conservative treatment and the patient was admitted to the hospital where a Magnetic resonance imaging (MRI) was done, which showed an extruded disc of L5-S1. The patient was also having weakness in the S1 myotome on the right.
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, dural tear, aggravation of the pain, deterioration of neurological status, non-recovery of the pain, repeat surgery, repeat disc herniation and possible need for fusion in the future among others.
We discussed systemic complications including blood clot, cardiac, pulmonary, and neurological complications including blindness and death. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The patient was flipped prone on a Wilson frame on a four-post Jackson table. All the bony prominences were well padded. The lower back was prepped and draped aseptically in the usual fashion.
Time-out was called. Preop antibiotic in the form of 2 g of Ancef was given. A spinal needle was passed in the area of interest. Fluoro was brought in and a lateral spot x-ray was done, which showed us at the level of L5-S1 intervertebral space.
With sharp and blunt dissection, the skin, fascia and posterior interspinous ligament was cut in the line of incision. Paravertebral muscles were dissected and retracted laterally with the use of Bovie on the right side of the spinous process. The lamina of L5 was reached.
A fluoro was brought in and Woodson was put under the lamina of L5 and x-ray was taken to confirm our level. Once the level was confirmed, laminotomy of the right L5-S1 was performed with the use of high-speed drill. Once the laminotomy was performed, ligamentum flavum was seen.
The ligamentum flavum on the right side of L4-L5 was removed to expose the nerve root. The nerve root was retracted medially with the use of Love nerve root retractor. The herniated disc could be seen. The extruded disc was removed with the use of pituitary and nerve hook in multiple attempts.
Further annulus was cut with the use of a sharp blade and partial discectomy was performed with the use of pituitary. The specimen was saved for histopathology. Further examination with the nerve hook and Penfield showed good decompression of the nerve root with no residual fragments.
Foraminotomy of Rt S1 was done with kerrison 3 & 4 mm. The Rt S1 nerve root was released from nearby adhesions with the use of nerve hook and Penfield 4. Good decompression was achieved. The wound was thoroughly irrigated. A 40 mg of Depo-Medrol mixed with Surgiflo was put in the area.
Closure of the fascia was done with the use of 0-Vicryl. A 1 g of vancomycin was instilled into the wound. Closure of the wound was done with the use of 2-0 Vicryl and 4-0 Monocryl. Dressing was done with the use of dermabond and steristrips. The patient was flipped supine, extubated and moved to recovery in a stable condition.
Patient was seen in 2 weeks status post right L5-S1 laminotomy, Right L5-S1 microdiscectomy, right L5-S1 epidural injection depo medrol. During their last follow up the patient stated that the radiculopathy was resolved.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
