The patient had been seen by us for an extended period of time with complaints of low back pain and pain radiating down to both legs, but more on the right side. He also had weakness in both lower extremities along with involvement of bladder. He had been seen by urology who was suggestive of it being of spinal origin.
Prior physical examination of the lumbar spine supported the diagnosis of lumbar canal stenosis. His imaging showed grade 1 to grade 2 spondylolisthesis with instability over L4-L5 with compression of nerve roots. There is also lateral recess compression at L3-L4 on the right and left side with compression of the traversing L4 nerve root.
We discussed treatment options in detail in the office as well as in the surgical holding area. We discussed infection, bleeding, possibility of CSF leak, injury to adjacent nerves and vessels, neurological deterioration, failure of implants, failure of healing, need for repeat surgery, need for antibiotics if anything gets infected, and the need for rehabilitation. We also discussed systemic complications including blood clots, cardiac, pulmonary or neurological complications including death.
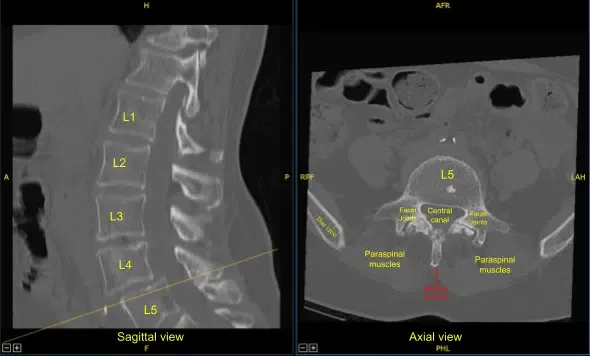
Preoperative CT of Lumbar Spine
The patient also understood and signed an informed consent to continue with the plan of decompression of L3-L5 along with an instrumented posterior spinal fusion of L4-L5.
The patient was taken to the operating room where general anesthesia was induced. The IV lines were secured. A Foley catheter was passed. Intraoperative neuromonitoring was put in place. The patient was turned prone on a four-post Jackson table with all bony prominences well padded.
Both shoulders were in a good position and well padded. The area of surgery was cordoned and cleaned and draped in the usual aseptic fashion. A time-out was called.
A midline incision was planned. The incision was carried deep into the spinous process and on either side of the spinous process with the help of bovie. The levels were checked. Further dissection was performed to expose the L3 and L4 lamina and the superior part of L5 lamina. The dissection was carried laterally to find the L4 and L5 transverse processes on either side.
Finally, it was decided to keep the median tension band intact and foraminotomy and laminotomy was performed on either side at L4 and L3 levels. The inferior facet of the L4 on the right side was removed to open the disc space.
The dura was unhealthy and thin and was having a lot of engorged vessels as well as scarring especially on the L4 level. The dura could not be separated easily. With the fear of durotomy and also it was found by the primary spin of the navigation arrow that the spondylolisthesis was well reduced that we decided not to perform the transforaminal interbody fusion.
The spin was performed by the navigation with the frame on. Once the dissection was done, we planned to find the screw holes first. Navigation probe followed by drill was used on the right and left L4 and L5 pedicles under navigation.
The screw holes were tapped. Pedicle probe was put in all the four holes. The screw was planned to be inserted in the end. Now, the decompression was further achieved on the right and left L3 and L4 laminectomies and foraminotomies leading to neurolysis of right and left L4 and L5 nerve roots.
In the process of decompression, there was incidental durotomy on the left L3 level. The durotomy was cordoned and secured. The nerve roots were put back into the thecal sac and primary closure of the durotomy was performed using Prolene #6-0. It was a watertight closure. A Valsalva maneuver was performed by increasing a pressure of 40 mm of HG and holding it for 20 seconds. There was no leak at that time.
Once that decompression was complete, the durotomy was sealed with the muscle flaps followed by DuraSeal and Surgicel in layers. Finally after the decompression, the screws were put in right and left L4 and L5 pedicles.
The transverse processes were decorticated using the bur on the right and left L4 and L5. A mixture of local bone with cancellous autograft with DBX and ViviGen was made and put into the lateral gutters between L4 and L5. The left L4-L5 facet joint was decorticated to allow fusion.
The wounds were thoroughly washed. Vancomycin 2 g was instilled into the wound. Surgical incision was closed in layers appropriately.
Bone marrow aspirate was also taken from the left iliac crest and mixed with the bone graft and was put into the lateral gutters. Final spin was taken with the navigation and found that the screws were in good place.
Once the closure was done, the patient was turned supine onto the bed. The patient was extubated. It was planned to send the patient to the floor with Foley in. The patient remained on bed rest for 48 hours.
Patient was followed in our office on regular intervals of 2 weeks, 6 weeks, 3 months and 6 months thereafter with gradual return of function. Physical therapy was also started. Patient did well postoperatively
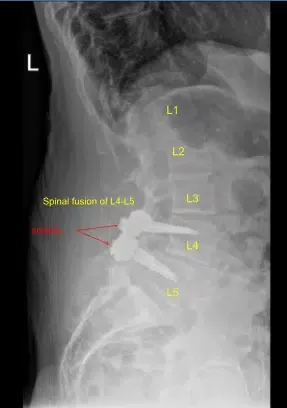
Spinal Fusion of L4-L5
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
