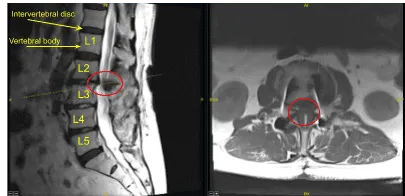
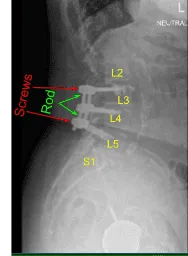
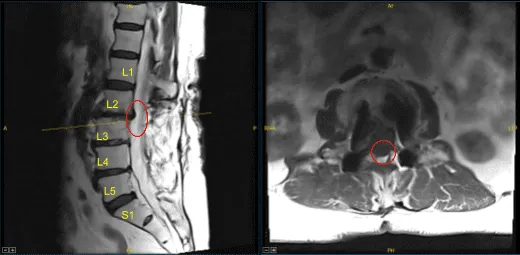
This patient had previously undergone an instrumented arthrodesis at an outside facility at L3-5. They presented with right anterior thigh and left posterior leg pain. Imaging displayed adjacent segment degeneration above and below her fusion mass which correlated well with her symptoms.
The patient was brought into the operating room and general endotracheal intubation was induced uneventfully. After successful induction of general anesthesia, the patient was positioned prone on the Allen table. All pressure points were inspected and padded appropriately.
The surgical area was then prepped and draped in the usual sterile fashion. Two separate midline incisions incorporating her prior midline spinal incision, were marked under fluoroscopic guidance. The incision was instilled with local anesthetic.
Beginning with the rostrally placed incision which overlies the L2-3 level, a #10 skin scalpel was used to incise the skin. Monopolar cautery was used to incise the subcutaneous layer and the fascia.
Electrocautery was used to remove the paraspinal musculature from the L2 lamina in a subperiosteal fashion, exposing the entirety of the L2 lamina to the lamina-facet junction. The inferior border of the L2 lamina was developed with an ongoing curette. The L2-3 level was again confirmed using lateral fluoroscopy.
At this stage, using a high speed midas rex drill starting with the right side, a bone window was created meticulously from the spinolaminar junction to the lamina facet junction and extending rostrally past the attachment of the ligamentum.
Boney edges along the perimeter were removed using 2mm and 3mm Kerrison rongeurs initially above the ligamentous plane. The ligament was then carefully removed with Kerrison rongeurs while paying close attention to the underlying dura. The decompression was carried through to the L2-3 foramina on the left side.
This process was then repeated on the left side. Residual scar from the prior operation was encountered caudal to the L2 lamina and was carefully removed with Kerrison rongeur along the medal L2-3 facet border after a plane was developed with up going curettes. In this fashion the L3-4 proximal foramina were decompressed bilaterally.
At this stage attention was then turned to the caudal midline incision which was opened sharply and taken down with monopolar electrocautery and Cobb elevators. This incision, though taken over the prior midline scar, was centered over the right L4-5 facet and right L5 pedicle screw tulip head which was clearly visualized. The level and position was confirmed with AP fluoroscopy.
The lamina and pars of the L5 level on the right side were exposed as was the L5 spinolaminar junction and lamina facet junction. In the same manner as above, a right sided L5 laminoforaminotomy was performed with a high speed midas rex drill, and a combination of curettes and Kerrison rongeurs. This was carried out to the extent that the traversing root of right S1 was seen and decompressed into the proximal foramina. The right L5 foramen was also decompressed.
A final AP and Lateral fluoroscopy image was obtained with opaque markers at all decompressed levels and foramina. The wound was irrigated then copiously with antibiotic impregnated saline. Duramorph was placed over the nerve roots after hemostasis was achieved. Plastic surgery was called for a complex multilayered wound closure.
At the end of the closure, the counts were confirmed to be accurate by the operating room staff. Dressings were applied. The drapes were removed and the patient was returned to a supine position for extubation.
The patient followed up 10 days after their surgeries and showed signs of gradual improvement. The patient then continued to follow up 2, 4 and 6 weeks after the surgery. The patient had reported improvements with their radiculopathy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 7, 2025.
