A patient who started having hand weakness and dexterity issues along with imbalance for the last one month. They had retention of urine with overflow incontinence. They had not been able to walk for one month. They have not been able to use their hands for activities of daily living. They felt that they had worsened and had then stabilized. They have had no recovery until now.
An MRI was done and found to have severe stenosis on C3-4 with moderate to severe stenosis on C4-5 and C5-6. Dr. Mariwalla and I discussed treatment options and the patient opted for surgical management. We discussed the need for anterior cervical discectomy and placement of cages as well as screws.
We also discussed regarding risks and benefits as well as complications including bleeding, infection, injury to adjacent nerves and vessels, aggravation or worsening of the problem, the need for ICU care, need for rehabilitation, failure of implant in future, need for surgeries, need for posterior surgery to back up incase the stability is not there.
Adjacent segment disease involving the proximal of the distal discs, systemic problems like blindness, paralysis, cardiac, neurological, pulmonary events, deep venous thrombosis, among others. The patient understood and signed the consent.

The patient was taken to the operating room where general anesthesia was induced. Multiple IV lines were put in. SSEPs and MEPs were set up by the electrodiagnostic team. The patient was moved onto the Jackson bed in a supine position. A roll was put between the shoulders.
The head was put on a donut and taped to the bed. The neck was prepared after clipping of hairs aseptically and draped. IV antibiotics were given to start up the procedure. Time-out was called.
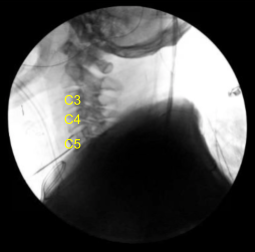
A transverse incision on the right side of the neck was planned, centered over C4 vertebra. C-arm was used to localize the level. A transverse incision of about 5 cm was given over the right side of the neck. Hemostasis was achieved.
Platysma was incised in line with the incision. Subcutaneous and subplatysmal dissection was done. Interval was formed between the sternocleidomastoid and the strap muscles. With the blunt dissection was created using a finger and Kittner a plane.
The carotid could be followed deep to the sternocleidomastoid laterally. The midline vertebra was reached and longus colli could be seen. Medial structures were dissected medially using hand-held Cloward’s. The lateral structures were dissected laterally with the hand-held Cloward’s.
Disc space was localized and marked with the spinal needle. C-arm was used to locate the level and found to be C4-5. The C-arm was removed and the disc space was marked with the Bovie for localization. Now, midline dissection was performed by raising the longus colli on either side from the lower C3 to the upper C6.
After very good exposure, the Caspar pins were inserted into the body of C3 and C4. Retraction was done using the self-retaining retractors. Skyline was used to dissect medially and laterally. Once the adequate reduction was achieved, the C3-4 disc was excised using curettes as well as 5-mm round bur. Once the disc was excised the posterior body was reached. The PLL and the disc were seen. The whole disc was removed along with the excision of PLL, right from the inferior C3 to the superior C4.
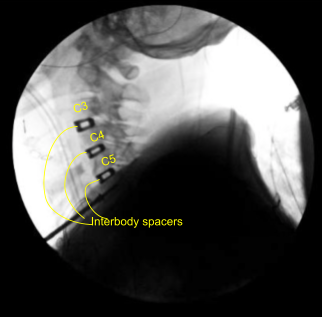
Bilateral foraminotomies were done using Kerrison punch 3.0. All the discs were thoroughly decorticated to achieve fusion. Once adequate foraminotomy and discectomy was done, a spacer was inserted to size the disc. After sizing, 8-mm Globus titanium cage filled with titanium interbody spacer, filled with autologous bone graft, mixed with Trinity and DBX was inserted finding it in adequate position.
Attention was moved to the C4-5 disc space. Caspar pin was inserted into the C5 body and expansion of C4-5 done with a self-retaining retractor. Skyline was moved inferiorly to retract medially and laterally. Discectomy was done in a similar fashion followed by excision of the posterior longitudinal ligament and bilateral foraminotomies. After adequate excision the sizing was done, Globus titanium spacer filled with Trinity and autologous bone graft and DBX was inserted again.
Again, a new pin was inserted into the C6 body and similar discectomy was done using curettes,matchstick bur and Kerrison punches. PLL was also excised. Bilateral foraminotomies of C5-6 was performed. A matchstick bur was used each time to make holes into the end plates for better fusion.
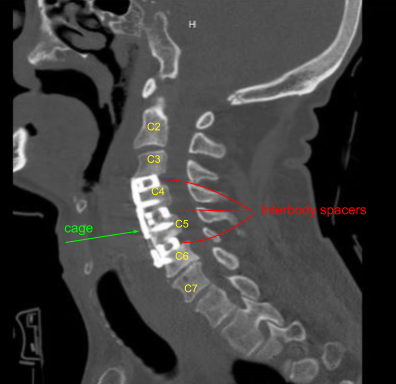
The cage was inserted, again packed with autologous bone graft, Trinity and DBX. After inserting all the three cages, the bony contouring was done using matchstick bur and plate was put of an adequate size. The plate was found to be adequate in AP and lateral views in a satisfactory position.
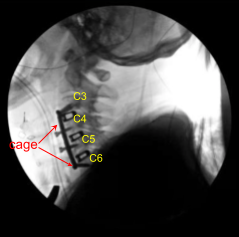
The plate was fixed using locking variable angle screws in the body of C3, C4, C5, and C6. Final pictures were taken and saved. The wound was thoroughly washed and hemostasis was achieved. The retractors were removed. Closure was done in layers using #2-0 Vicryl and Monocryl. Dressing was applied.
A hard cervical collar was put on the patient. There were no neuromonitoring incidents during the surgery. The patient was extubated and moved to the recovery unit in stable condition. The patient initially followed up 10 days after their surgery and then continued to follow up 2, 4, 6, 8, weeks after the surgery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
