This Patient presented to the outpatient clinic with signs and symptoms of cervical spondylotic radiculopathy. Having failed extensively with nonsurgical treatments with progressively severe pain syndrome, surgery was recommended to decompress and stabilize the cervical spine.
The risks, benefits, alternatives and potential complications of the surgery were explained to them. All questions were answered until no further issues were raised and they provided written informed consent which was placed in the chart.
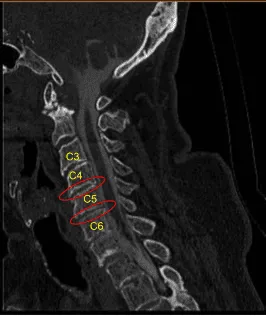
Cervical Spondylotic
The patient was brought to the operating room. Their identity was verified. General anesthesia was induced. They were intubated by the Anesthesia Service. Respiratory and cardiac monitoring leads were placed. Neuromonitoring leads for somatosensory evoked potentials and EMG were placed.
They were positioned supine on the operating room table with the head in mild extension and the shoulders gently taped down for fluoroscopic visualization. Fluoroscopy was used to localize the C5 index level. Skin was cleaned with chlorhexidine. A transverse incision was demarcated on the right side.
Skin was sterilized with a DuraPrep solution. They received preoperative prophylactic IV antibiotics. Surgical timeout was performed. Sterile drapes were placed in the usual manner. 2% lidocaine with epinephrine was infused along the incision line
The skin was opened with a #10 blade scalpel. Hemostasis was obtained with bipolar electrocautery. Metzenbaum scissors were used to undermine the platysma which was divided sharply with the Bovie. Omohyoid was released with the Bovie.
Blunt dissection and Cloward handheld retractors were used to approach the anterior cervical spine. Kittners were used to sweep the prevertebral fascia. A spinal needle was placed into the C5-C6 interspace. The C-arm unit was draped sterilely, brought into the field and used to confirm the level.
Bovie monopolar was used to expose the anterior cervical spine from C4 to C6 undermining bilateral longus colli muscles. TrimLine self-retaining retractor system was placed. Caspar pins 12 mm were placed into the C4, C5 and C6 anterior vertebral bodies. Gentle retraction was applied first across C5-6.
Annulotomy was performed with a #15 blade scalpel. Osteophytes were retracted with electric high-speed drills and Kerrison rongeurs. Autograft from bone morselization was collected with Penfield instruments and added to the demineralized bone matrix allograft for arthrodesis.
Discectomy was performed with curettes and pituitary rongeurs. Electric high-speed drill was used to expose the posterior longitudinal ligament which was entered with a nerve hook and retracted in a piecemeal fashion with Kerrison rongeurs exposing the intact dura.
Bilateral foraminotomies were performed with Metzenbaum-Penfield technique and Kerrison rongeurs to neurolyze and decompress the bilateral C6 nerve roots. Hemostasis was obtained with Surgiflo hemostatic matrix, thrombin soaked Gelfoam, and cottonoids.
Distraction was then applied across C4-5. Similarly, an annulotomy was performed with a #15 blade, discectomy with curettes and pituitary rongeurs, collection of autograft with Penfield, exposure of posterior longitudinal ligament with electric high-speed drill, preparation of endplates with curettes and drill, resection of PLL with nerve hook and Kerrison, bilateral neurolysis of C5 nerve roots with Penfield technique and foraminotomies with Kerrison rongeurs. Hemostasis similarly was obtained with Surgiflo hemostatic matrix, cottonoids, and thrombin soaked Gelfoam.
Trials were used to select a 7 mm lordotic titanium interbody spacer which was filled with morselized autograft and allograft and gently tamped into C4-5 and C5-6 interspaces with a mallet into the correct position. Caspar pins were removed. The bony defect was waxed.
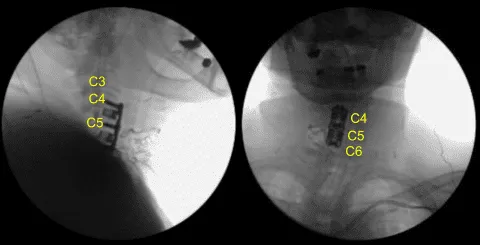
AP and lateral fluoroscopy showed correct positioning. Motor evoked potentials showed slight decrease in amplitude in the right C5-6. The instrumentation was then removed. The instrumentation space was cleaned out and irrigated flush.
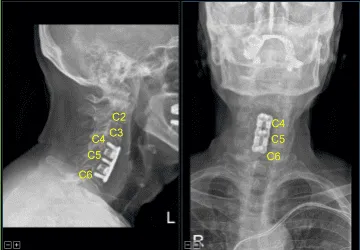
There was no significant change, so the interbody spacer was replaced. Anterior osteophytes were flushed with an electric high-speed drill. Hemostasis was obtained with bone wax. Titanium lordotic plate was placed from C4 to C6 and secured with a pin.
Fluoroscopy showed correct sizing and positioning, so it was secured with six 14 mm titanium screws decorticating with a handheld 12 mm electric drill. AP and lateral fluoroscopy showed good positioning. All the screws were final tightened using an integrated device in the plate.
The wound was irrigated clear. Hemostasis was confirmed with bipolar. Motor evoked potentials showed improvement and the signals were present in all four extremities. SSEPs were stable.
The closure was accomplished in layers with 3-0 Vicryl suture for the subdermal layer followed by 4-0 subcuticular Monocryl for the skin, followed by sterile cleaning and dressing with Dermabond glue. A 7 mm Jackson-Pratt drain was placed through a separate skin incision and secured with 3-0 nylon suture.
The patient was transferred to the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient initially followed up two weeks after the surgery and then continued following up in our office periodically. In their visit the patient stated that they had experienced improvements with their radiculopathy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
