The patient presented to neurosurgery clinic with signs and symptoms of cervical spondylotic myelopathy, cervical stenosis and cervical spondylolisthesis at C7-T1 with lower extremity weakness, loss of dexterity and early signs of myelopathy as well as cord signal changes on the MRI imaging.
Surgery was recommended to decompress and stabilize the cervical and thoracic spine. Risks, benefits, alternatives and potential complications were explained to the patient and all their questions were answered until no further issues were raised. They provided written and informed consent and were placed in the chart.
The patient was brought to the operating room and their identity was verified. General anesthesia was induced. They were intubated by the anesthesia service. Respiratory and cardiac monitoring leads were placed.
Neuromonitoring leads for motor evoked potential, somatosensory evoked potential and EMG were placed. Baseline signals were obtained showing no motor evoked potential responses in the lower extremities. The patient was known to be wheelchair bound already with bilateral foot drop, so it correlated.
Their head was placed in Mayfield three-point pin fixation. Foley catheter was placed. They received preoperative prophylactic IV antibiotics 3 gm of cefazolin IV. They were positioned prone on a Jackson Relton-Hall frame.
Mayfield clamp was affixed to the Mayfield adapter. All pressure points were carefully padded. Posterior cervical and thoracic area were prepped with an electric hair clipper and cleaned with chlorhexidine.
Airo CT scan was performed. Skin was sterilized with a DuraPrep solution. Sterile drapes were placed in the usual manner. A spinal needle was brought to the field and localized. 1% lidocaine with epinephrine was infused.
The skin was opened with a 10-blade scalpel. Hemostasis was obtained with bipolar electrocautery. Cobb elevator and Bovie was used to carry the incision down through the subcutaneous tissues, sharply divided the fascia and exposed posterior elements of the cervical and thoracic spine from C5 to T2.
Self-retaining retractors were placed. Hemostasis was obtained with bone wax, Bovie and bipolar cautery. Neuronavigation array was affixed to the spinous process, clamped to the T1 spinous process. The patient was draped. CT scan was obtained, and data transferred to the neuronavigation computer, and accuracy verified.
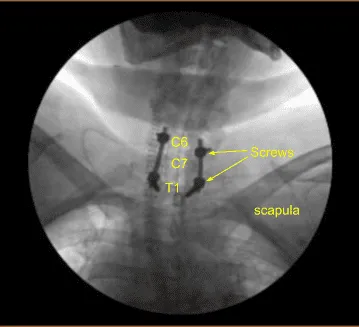
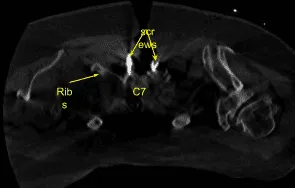
Image-guided stereotactic frame with neuronavigation techniques were used to place the instrumentation. We placed bilateral T1 pedicle screws and decorticated with electric high-speed drill cannulating with the navigated pedicle finder, palpating for breaches, measuring the depths, under tapping by 11 mm and placing 30 mm x 5.0 mm titanium pedicle screws bilaterally without difficulty.
Motor evoked potentials were checked periodically and were stable. Next, we cannulated the bilateral C5 and C6 lateral masses using navigation technique, decorticating with electric high-speed drill, cannulating with a 12-mm drill guide and electric hand-held drill, palpating for breaches, filling the hole with Surgiflo.
Next, we performed C6, C7 and T1 laminectomy by drilling bilateral troughs under continuous sterile irrigation and resecting the C6, C7 lamina en bloc with Leksell rongeur. We then resected residual bone and hypertrophic ligamentum flavum with various Kerrison rongeurs carefully protecting the dura.
The dura was inspected and was intact without any sign of CSF leak or durotomy. Motor evoked potentials were checked and showed an improvement with responses apparent in the lower extremities that were not present before decompression.
Next, we placed bilateral lateral mass screws at C6. Inspecting the deformity of the spine, a decision was made not to place the C5 lateral mass screws because of kyphotic deformity and difficulty with rod placement.
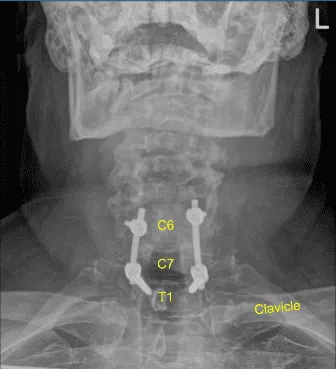
So, we next decorticated the joints at C6-C7 and C7-T1 and bilateral T1 transverse processes with electric high-speed drill for the arthrodesis. The autograft resected was morselized. Precut-precontoured titanium rods were placed across the tulips from C6 to T1 and secured with locking caps and then final tightened with a torque and anti-torque device.
Morselized autograft and demineralized bone matrix allograft was packed in lateral gutters from C6 to T1 bilaterally. The wound was irrigated copiously until clear. Hemostasis was confirmed.
Vancomycin powder was applied. A medium-sized Hemovac drain was tunneled in a subfascial manner and secured to the skin with a 3-0 nylon suture. The fascia was closed in a watertight manner with 0 Vicryl sutures and an additional layer of 0 Vicryl sutures was placed due to the patient’s habitus.
Exparel long-lasting local anesthetic was infused in the soft tissues. Subdermal layer was closed with interrupted 2-0 Vicryl sutures and the skin was reapproximated with surgical staples, cleaned and dried sterilely, and dressed with Mepilex bacteriostatic dressing. Hemovac canister was applied to suction. Mayfield clamp was released with the adapter.
The patient turned supine on the cart. Mayfield clamp was removed. The patient was extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient initially followed up in 16 days after the surgery and then continued following up in our office 4, 6, 8, 12, 24 weeks. In their last office visit the patient stated they were able to do their usual activities. They also stated that physical therapy was going well and signs of myelopathy were resolved.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 7, 2025.
