A patient presented to our clinic with signs and symptoms of severe lumbar stenosis. Surgery was recommended to decompress his lumbar spine after failure of conservative treatment measures.
The risks, benefits, alternatives and potential complications were explained to them. All his questions were answered until no further issues were raised and they provided written informed consent.
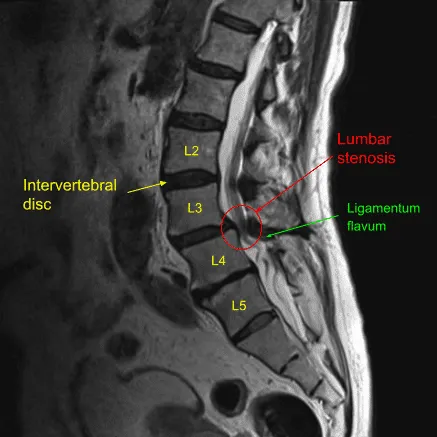
Sagittal view of pre-operative Lumbar Spine MRI
The patient was brought to the operating room. their identity was verified. General anesthesia was induced. The patient received prophylactic IV antibiotics. Neuromonitoring leads for somatosensory evoked potential and EMG were placed. The patient was positioned prone on a Wilson frame and all pressure points were padded. Lumbar area was cleaned with chlorhexidine, sterilized with
DuraPrep solution, and sterile drapes were placed in the usual manner. C-arm unit was draped sterilely, and the microscope was balanced and draped sterilely and the procedure was performed using microsurgical instruments and technique.
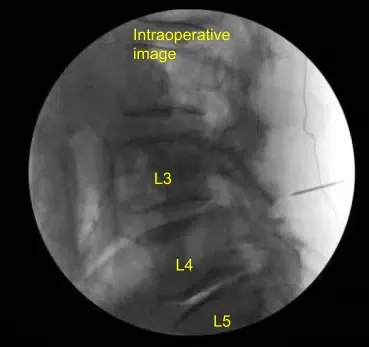
Spinal needle was used to localize the L4-L5 level on the right side. A 1.8-cm linear incision was demarcated and infiltrated with local anesthesia. Skin was opened with a 10-blade scalpel. Hemostasis was obtained with Bovie and Bovie was used to sharply divide the fascia. Sequential dilators were used to dock an 18-mm x 5-cm tubular retractor which was affixed rigidly to the bed frame.
Microscope was brought into the field. Soft tissue overlying the lamina was resected with Bovie and pituitary rongeurs. Right L4 laminotomy was performed with electric high-speed drill with continuous Cefazolin infused sterile irrigation.
Bone wax was used for bone bleeding but there was very little. Ligamentum flavum was detached from cephalad point and reflected caudally with micro angled curette and then resected in piecemeal fashion with Kerrison rongeurs.
Ligamentum flavum was severely hypertrophied correlating with the preoperative imaging. Once verified it was complete, the bed was air planed and the tubular retractor was angled to the left side contralateral over the top. Laminotomy was performed on the left side at L4-L5. Dura was carefully protected with cottonoids while contralateral hypertrophied ligamentum flavum was resected.
Hemostasis was confirmed with a surgical hemostatic matrix. The wound was irrigated clear. No durotomy was Identified. Microscope and tubular retractor were removed after confirming hemostasis with bipolar electrocautery.
The fascia was closed in a watertight fashion with interrupted 2-0 Vicryl sutures and then Exparel anesthetic was infused in the soft tissues. Subdermal layer was closed with 2-0 Vicryl interrupted pop-off sutures and the skin was reapproximated with the running subcuticular 4-0 Monocryl stitch, cleaned and dried sterilely and dressed with Dermabond glue followed by a Band-Aid.
The patient was turned supine on the cart, extubated uneventfully, and transported to the recovery room in stable condition. At the end of the case, all sponge count, needle counts, and instrument counts were correct, and the patient tolerated the procedure well with 5 cc estimated blood loss and no complications.
The patient initially followed up 14 days after the surgery and then continued to follow up in our outpatient clinic 4, 6, and 8 weeks after the surgery. The patient showed signs of gradual improvement with symptoms of severe lumbar stenosis. The patient has returned to doing daily activities with little to no pain.

The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
