A pleasant patient who was involved in a car crash and subsequently developed neck pain. They had lots of conservative treatments, but ultimately failed, and developed myelopathy with correlated imaging findings from C4 to C6. Therefore, we offered surgery. The patient gave informed consent, understanding all of the risks, benefits, and alternatives to surgery.
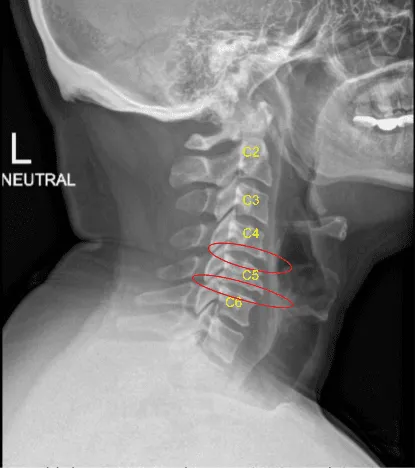
Mild degenerative changes C4-C5 and C5-C6
The patient was identified in the Preoperative Holding Area by two separate patient identifiers and then brought back to the Operating Room where they were induced under general anesthesia and intubated without incident.
Neuromonitoring electrodes were attached and tested. The patient was placed supine on to the Operating Room table with their head in a gel doughnut and a small interscapular bump placed to position the neck in a natural lordotic position.
We localized our incision using a radiopaque marker and traced the incision with an indelible marker from the midline of the trachea to the medial border of the sternocleidomastoid muscle on the patient’s right side. We then prepped and draped the neck in the usual sterile fashion, dosed IV antibiotics, and completed a call to order.
A #15 blade was used to incise the skin along the natural skin crease and thereafter reverse Metzenbaum technique was used to create a subcutaneous dissection plane. We then undermined the platysma muscle and cut it sharply using bipolar cautery to control bleeding.
Subplatysmal dissection was carried out with mosquito hemostats and reverse Metzenbaum technique. We followed the fascial plane on the medial border of the sternocleidomastoid muscle down to the fascia anterior to the spine, carefully retracted the esophagus and carotid artery out of view. We localized our level of operation using fluoroscopy.
We used handheld retractors to hold the skin and muscle edges apart and deflated the endotracheal cuff to just before a cuff leak. Undermining the longissimus muscle with Bovie cautery and freeing up the disc spaces from overlying tissues, we were then able to apply our self-retaining retractor set and completed our exposure of the disc spaces from C4 to C6.
There was significant osteophytic overgrowth and we removed this bone and flattened the anterior vertebral bodies using Leksell Rongeurs and the drill. We morselized and saved this bone for use later in the case.
At this point, we placed Caspar pins into the C5 and C6 vertebral bodies and applied gentle distraction. Using a combination of curettes, Kerrisons, rongeurs and pituitary rongeurs, we started our discectomy and applied gentle distraction as we continued our discectomy down to the posterior longitudinal ligament.
The disc was extremely degenerated at this level and we reached the posterior longitudinal ligament and undermined it and resected it using 2 mm and 3 mm Kerrison punches.
Posterior osteophytes were then removed with a drill and Kerrison punches then we created wide foraminotomies bilaterally. We followed the nerve roots out through the neural foramen using the blunt nerve hook freeing them from all compressive elements and mobilizing them.
Epidural bleeding was controlled easily with Surgiflo and gentle cotton tamponade. We then trial-sized our implant and obtained x-rays. We filled our implant with morselized allograft and morselized autograft.
We inserted it carefully under direct visualization and used x-rays to ensure appropriate placement. We removed the inserter and washed out the wound. We thereafter removed the Caspar pin from the C6 vertebral body and covered the hole with bone wax.
We transferred our attention to the C4 C5 disc space and frame-shifted our retractors cephalad. We inserted a Caspar pin into the C4 vertebral body, applied gentle distraction, and repeated the process here for discectomy and arthrodesis. Using a combination of curettes, Kerrisons, rongeurs and pituitary rongeurs, we started our discectomy and applied careful distraction as we continued our discectomy down to the posterior longitudinal ligament.
The disc was extremely degenerated at this level. We reached the posterior longitudinal ligament and undermined it and resected it using 2 mm and 3 mm Kerrison punches.
Posterior osteophytes were then removed with a drill and Kerrison punches and we created wide foraminotomies bilaterally and followed the nerve roots out through the neural foramen using the blunt nerve hook freeing them from all compressive elements and mobilizing them. Epidural bleeding was controlled easily with Surgiflo and gentle cotton tamponade.
We squared out the disc space with the high-speed drill and prepared the disc space for arthrodesis. We then trial-sized our implant and obtained x-rays. We filled our implant with a morselized allograft and a morselized autograft.
We inserted it carefully under direct visualization and used x-rays to ensure appropriate placement. We then removed the inserter and washed out the wound. We thereafter removed the Caspar pin from the C4 and C5 vertebral bodies and covered the holes with bone wax.
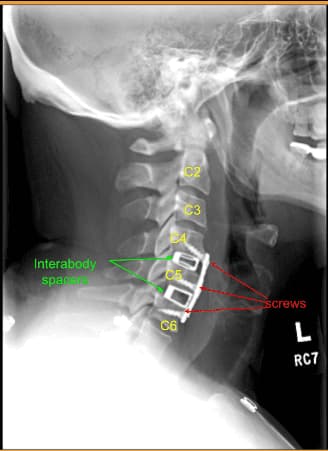
At this point we measured out our anterior plate, placed it over our levels of interest, and pinned it into place. We obtained x-rays, and then removed the plate and applied additional curvature to the plate to seat it appropriately against the anterior border of the vertebral bodies. We then replaced the plate and applied the screws as listed above. We locked all the screws in place and obtained final AP and lateral x-rays.
We then washed out the wound copiously with Bacitracin irrigation and used bipolar cautery to achieve meticulous hemostasis. We applied steroid paste to the retroesophageal space and closed the platysma muscle with a running #3-0 Vicryl stitch. The platysma was reapproximated using 3-0 running Vicryl.
The deep dermal layer was closed with inverted interrupted #3-0 Vicryl sutures and the skin was closed with a #5-0 running subcuticular Monocryl stitch. The incision was dressed with Steri-Strips and the patient was placed in a cervical collar prior to being transferred off of the Operating Room table extubated.
All counts were correct at the end of the case x2 and I was scrubbed for all portions of the case. There were no changes in neuromonitoring throughout the case. The patient was extubated in the operating room.
The patient initially followed up in two weeks after the surgery and then continued to follow up as an outpatient every 4, 6, 8 weeks. In their last office visit the patient stated they were well, able to do their usual activities and myelopathy had been resolved.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 17, 2025.
