Case Study: L4 to S1 Transforaminal Lumbar Interbody Fusion
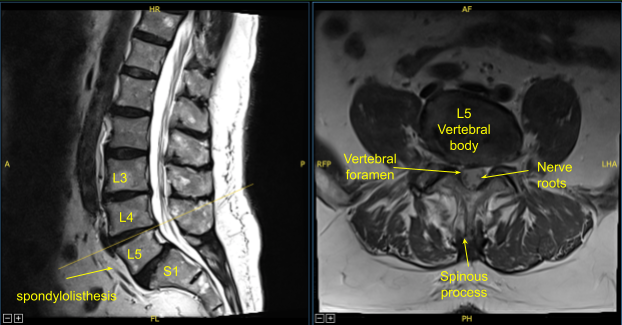
A patient presented to our clinic with signs and symptoms of lumbar spondylolysis, spondylolisthesis and spondylotic radiculopathy. Having failed conservative treatment measures, surgery was offered and recommended to decompress and stabilize the lumbar spine.
The risks, benefits, alternatives and potential complications were explained to him. All of their questions were answered until no further issues were raised and they provided written informed consent which was placed into the chart.
The patient was brought to the operating room. Their identity was verified. General anesthesia was induced. They were intubated by the anesthesia service. Respiratory and cardiac monitoring leads were placed. Neuromonitoring leads for somatosensory evoked potentials and EMG were placed and baseline signals were obtained.
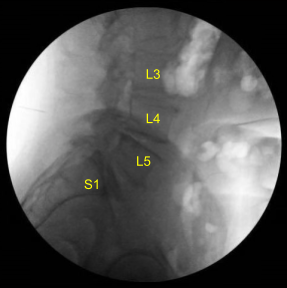
He was positioned prone on a Jackson Relton-Hall frame. All pressure points were carefully padded. They received preoperative prophylactic IV antibiotics, tranexamic acid and dexamethasone. Lumbar area was prepped with an electric hair clipper and cleaned with chlorhexidine. A 23-gauge spinal needle and fluoroscopy was used to localize the index level.
A midline incision was demarcated. Skin was sterilized with DuraPrep solution and sterile drapes were placed. 1% lidocaine with epinephrine was infused along the incision line.
Skin was opened with a #10 blade scalpel. Hemostasis was obtained with bipolar electrocautery. Bovie monopolar was used to carry the incision down through the subcutaneous tissues in the midline and sharply divide the supraspinous ligaments and fascia.
Cobb elevators and Bovie were used to perform subperiosteal dissection exposing the posterior elements of the spine including transverse processes of L4, L5 and S1. Allis clamp was affixed to the L4 transverse process.
The C-arm unit, which was draped sterilely, was brought into the field and used to confirm the level. Neuronavigation array was affixed to the right superior posterior iliac crest with two Schanz pins after infiltrating with local anesthesia and making #15 blade stab incisions.
The patient was sterilely draped. CT scan was obtained. Data was transferred to the neuronavigation computer. Accuracy was verified. Neuronavigation techniques were used to morselized bone for arthrodesis autograft. Leksell rongeurs, Kerrison rongeurs and electric high-speed drill under continuous sterile irrigation were used to perform complete L4-5 laminectomy and facetectomies, completely neurolyzing with Penfield-Metzenbaum technique the L4, L5 and S1 nerve roots.
Epidural bleeding was controlled with Surgiflo hemostatic matrix and bipolar electrocautery. Bone bleeding was controlled with bone wax. L4-5 and L5-S1 interbody arthrodesis was performed by retracting the thecal sac with a nerve root retractor, performing annulotomy with a bayoneted #15 blade scalpel.

Discectomy was performed with sequential paddle shavers and various pituitary rongeurs. Endplates were prepped for arthrodesis with scrapers, rasps and curettes. The patient was noted to have poor bone quality.
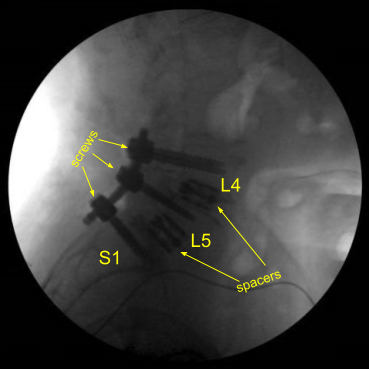
Expandable titanium interbody spacers, 15-degree lordotic at L5-S1 and 10-degree lordotic at L4-5, were placed under fluoroscopic guidance and expanded to proper fit. There was partial subsidence of the interbody spacer at L5-S1 into the L5 body, but it was secured and tight fit and imaging showed midline positioning.
CT scan was then obtained (shown above) which showed correct positioning of all the hardware. Neuromonitoring signals were stable. The wound was irrigated copiously. Bilateral transverse processes were decorticated for posterolateral arthrodesis from L4 to S1.
Morselized autograft, demineralized bone matrix and ViviGen allograft were packed into lateral gutters. There was also a bone graft both ViviGen and DBX packed into the interbody spaces with the spacers at L4-5 and L5-S1.Vancomycin powder was applied. Hemostasis was confirmed.
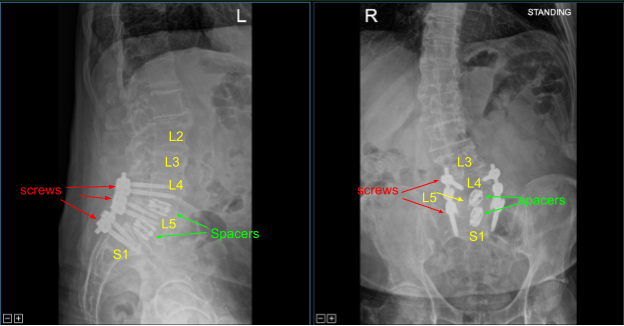
Precut titanium rods were contoured with rod benders and placed across the screw tulips from L4 to S1and secured with locking caps which were all final tightened with a torque and anti torque device. Final AP and lateral x-rays showed correct and complete hardware implantation.
The patient was then turned supine on the cart, extubated uneventfully and transported to the recovery room in stable condition. At the end of the case, all sponge counts, needle counts, and instrument counts were correct. The patient tolerated the procedure well.
The patient was followed up two weeks after their surgery and then continued to follow up in our office 4, 6, and 8 weeks after the surgery. The patient showed gradual signs of improvement with lumbar spondylolysis, spondylolisthesis and spondylotic radiculopathy.
Sagittal View Axial View
Post Op X-ray
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.

Dr. Nakul Karkare
I am fellowship trained in joint replacement surgery, metabolic bone disorders, sports medicine and trauma. I specialize in total hip and knee replacements, and I have personally written most of the content on this page.
You can see my full CV at my profile page.