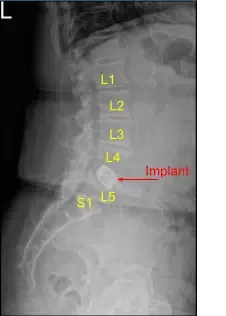
A patient who had previously undergone a L4/5 lateral interbody fusion, but ended up developing severe left leg radiculopathy and then moderate right leg radiculopathy, associated with severe piriformis syndrome.
They underwent conservative measures at first, but the pain was unbearable, so we ultimately offered them a posterior decompression. MRI of the lumbar spine revealed severe stenosis at L4 and L5 with a large disc protrusion. The patient also had pain unresponsive to IV pain medication.
Given osteoporosis and our concern for stability at L4/5 with endplate fractures at the previous L4/5 implant, we considered an instrumented fusion. The patient gave informed consent, understanding all the risks, benefits and alternatives to surgery.
The patient was identified in the preoperative holding area by two separate patient identifiers and brought back to the operating room where the patient was induced under general anesthesia and intubated.
Neuromonitoring electrodes were attached and tested and the patient was turned prone onto a Wilson frame attached to a Jackson table with all pressure points padded and the patient’s eyes free from pressure. The tablet was then placed in a slight reverse Trendelenburg position.
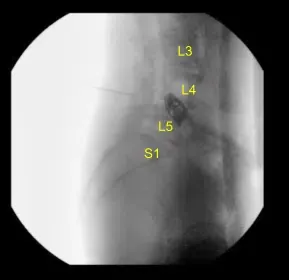
The lumbar region was prepped and draped in the usual sterile fashion and then employed a fluoroscopy to localize our incision, which was traced with an indelible marker on the midline of the lumbar region overlying the L4-L5 interspace. IV antibiotics were dosed and a call to order was completed.
A #10 blade was used to incise the skin down to the level of the subcutaneous fat and thereafter, Bovie cautery was used to continue the dissection down the midline avascular plane preserving the supraspinous and interspinous ligaments and following the subperiosteal plane exposing the L4 and L5 laminae.
We removed the soft tissue from the bone in a nontraumatic fashion and then applied the McCullough retractor system. Then the right-angled Gelpi retractors were used to hold the skin and muscle edges apart. We used fluoroscopy once again to localize our level of operation.
A 3 mm drill bit was attached to the electric drill and used to create wide laminectomies at the L4/5 level and laminotomies bilaterally. Once the ligamentum flavum was encountered, we used Kerrison punches bilaterally to remove the extra bone fragments and to complete medial facetectomies and foraminotomies.
The ligamentum flavum was then undermined with curette and removed with Kerrison punches. We created a wide foraminotomies for L4 and L5 nerve roots bilaterally and followed the course from their exits from the thecal sac out of the neural foramen circumferentially using a blunt nerve hook and ensuring that they were free from all compressive elements.
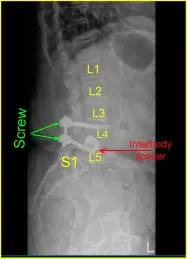
The nerve roots were gently retracted on both sides to access the L4/5 disc space. Here, we are able to access the disc space and mineralized components of the disc were removed with pituitary rongeurs. At this point, we explored the disc space thoroughly and washed out any fragments until we reached the interbody device, ensuring that the thecal sac and nerve roots were completely decompressed.

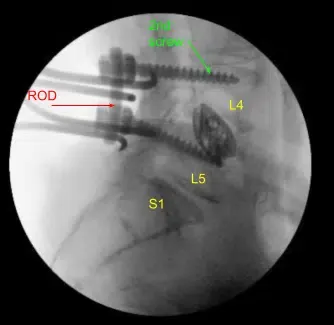
Given the concern for the implant in the prone position and our feeling that the endplates may have fractured more, we exposed the transverse processes for L4 and L5 and used the drill to create pilot holes in the pedicle on the left side at L4 and L5. Under fluoroscopy, we guided probes through the pedicles and tapped each pedicle, then placed pedicle screws into L4 and L5.
These screws were stimulated, and checked under fluoroscopy, and then a rode was placed and cap screws were given a final tightened. On the right side and left side, we decorticated the facets and transverse processes and placed our fusion mass for arthrodesis.
Bleeding was controlled easily with bipolar cautery and Surgiflo followed by gentle cotton tamponade. We added a tiny amount of duraseal for concern of thin dura and to prevent a CSF leak. We then washed out the wound copiously with bacitracin irrigation and applied the steroid paste onto the nerve root followed by vancomycin powder. The paraspinal muscles were disinserted and rotated medially after finding the blood supply.
These muscles were closed at the level of the muscle and fascia with 0 Vicryl sutures. A small fascial advancement flap was then created and the fascia was closed with 0 Vicryl sutures and the dermis was closed with #2-0 Vicryl sutures in an inverted interrupted fashion.
The skin was then closed with a 4-0 running subcuticular Monocryl stitch and dressed with Dermabond and a sterile dressing. All counts were correct at the end of the case x2 and the neuromonitoring signal remained stable throughout the case.
The patient initially followed up 12 days after their surgery and then continued to follow up 4, 6, and 8 weeks after their surgery. They had stated their left and right leg radiculopathy had been resolved. They were able to return to their daily activities.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
