An 82-year-old male presented to our office with worsening pain in the bilateral hips and groin areas. The patient was a retired school teacher. He was currently staying with her daughter and was in the ER last year for hip pain. The pain has been bothering him for the past five years.
The pain started gradually and was moderate to severe in intensity. The patient describes the pain as sharp to dull ache located in both groins (left greater than right). The pain was especially worse on walking and recently made him dependent on a rolling walker.
He was a former smoker (20 pack-years) having quit 10 years ago. He had a cardiac catheterization 4 years ago and bilateral arthroscopic shoulder surgery 2 years ago. The patient was being treated for coronary artery disease, peripheral artery disease with a stent in the right political artery, dyslipidemia, and hypertension.
He had previously tried conservative management in the form of physical therapy, heat pads, and cortisone injections but without sustained relief. The patient stated he felt depressed owing to his reduced mobility and pain.
On his office visits, the physical examination revealed a steady, coordinated antalgic gait with reduced stance phase on the left side. There was a left anterior hip joint line tenderness on deep palpation. Extension, abduction and internal rotation movements were restricted and painful.
The skin overlying the left groin was normal with no scar, sinus or erythema. There was no fullness in the Scarpa’s triangle. Both the anterior superior iliac spines were at the same level with no exaggeration of lumbar lordosis. There was absence of any functional or structural scoliosis.
The examination of bilateral knees, ankles was normal with mild restriction of range of motion on the right hip. There was no distal neurological deficit and bilateral lower extremity pulses were good volume. The patient denies any bowel bladder abnormality. He denied any history of long term alcohol abuse and steroid abuse.
Imaging study revealed bilateral arthritis of the hip joint. There were severe degenerative changes on the left hip. After careful consideration of his cardiac risk factors, he was advised left total hip arthroplasty. Risks, benefits, and alternatives were discussed with him at length. He agreed to undergo left hip replacement.
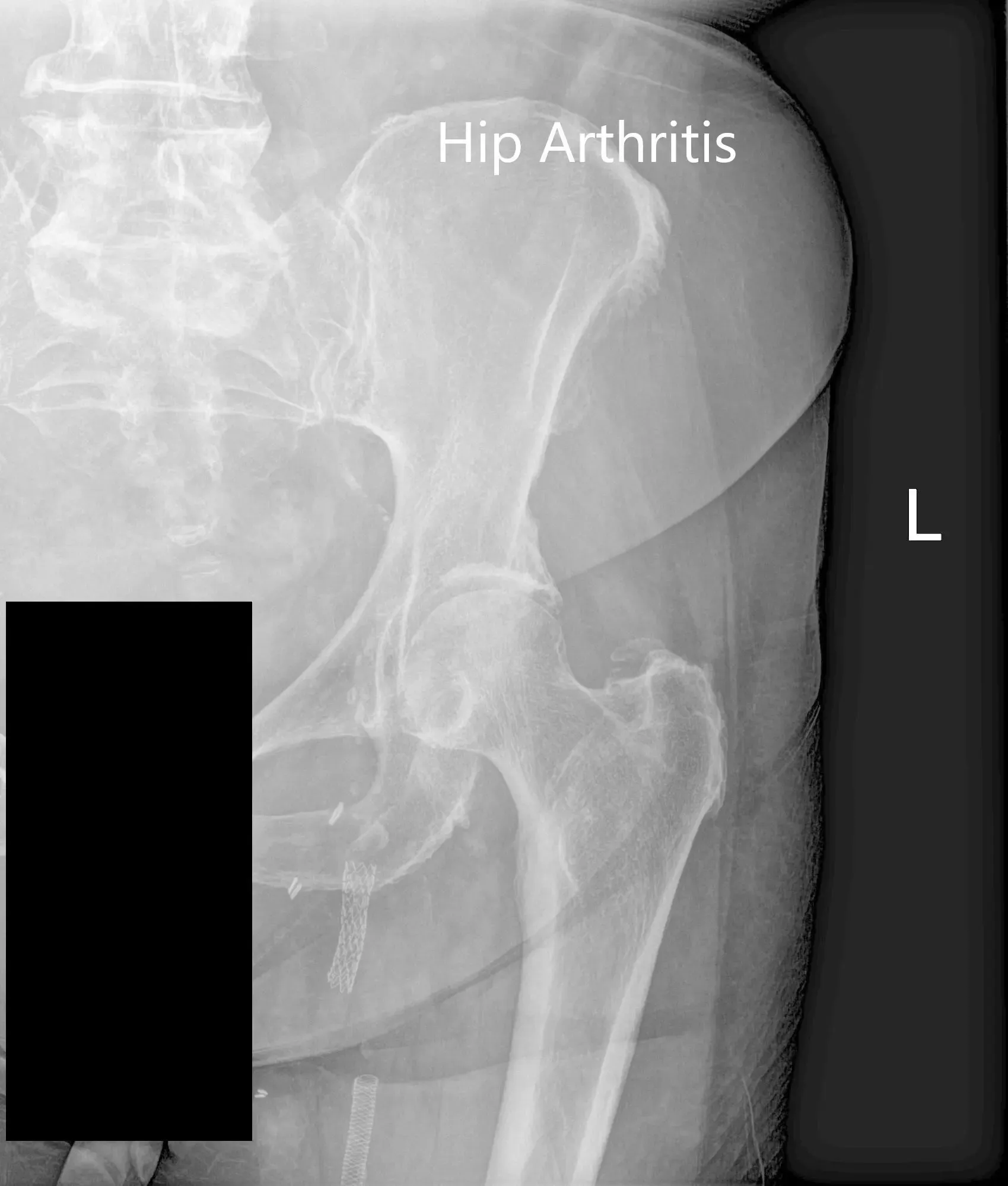

Preoperative X-ray of the left hip showing AP and frog-leg lateral views
Operation: Left total hip arthroplasty
The implant used: Titanium hemispherical shell 60 mm with a 6.5 cancellous screw, 6.5 mm in diameter, 25 mm in length with ceramic femoral head 36 mm, 0-degree polyethylene with 127-degree neck angle hip stem size 5.
Description of the procedure: The patient was brought to the operating room after obtaining informed consent and signing the correct surgical site. The risks, benefits, and alternatives were extensively discussed with the patient prior to the procedure. The patient was brought to the operating room and anesthesia was obtained by the anesthesiologist.
The patient was definitively positioned with the left hip up and the left hip was then draped and prepped in the usual sterile manner. The straight incision centered over the greater trochanter was used for the arthrotomy. Skin and subcutaneous tissues were then incised. The fascia was then divided. The robotic arm images were used for the planning of the surgery.
The acetabulum was then exposed. The remainder of the labrum was then debrided. The acetabulum was reamed and the final shell was then placed into position in the correct abduction and anteversion.
The shell was then placed over the cup after the placement of the screw. Attention was then turned towards the femur. The remainder of the tissue on the undersurface of the greater trochanter was then removed. The femur was then sequentially broached and the final broach was left into position.
The trunnion was then placed over the shell and the head was then placed over the trunnion. The pre-robotic plan was used in the assessment of the height. The lesser trochanter to center distance was also measured preoperatively before making the neck resection and was also compared after placement of the trial component. The hip was then reduced and trialed through a full range of motion and the hip was stable in all physiological range of motion.
The hip was dislocated. Trial components were then removed. The final components were then placed into position. The hip was then reduced again. A thorough lavage was given. The posterior soft tissue structures were then tacked to the greater trochanter through transosseous tunnels. Thorough lavage was given.
The fascia was closed, cutaneous tissues were closed, subcutaneous tissues were closed. The skin was closed using staples. Sterile dressing was then applied over the wound and the patient was then transferred to the postoperative care unit in stable condition.
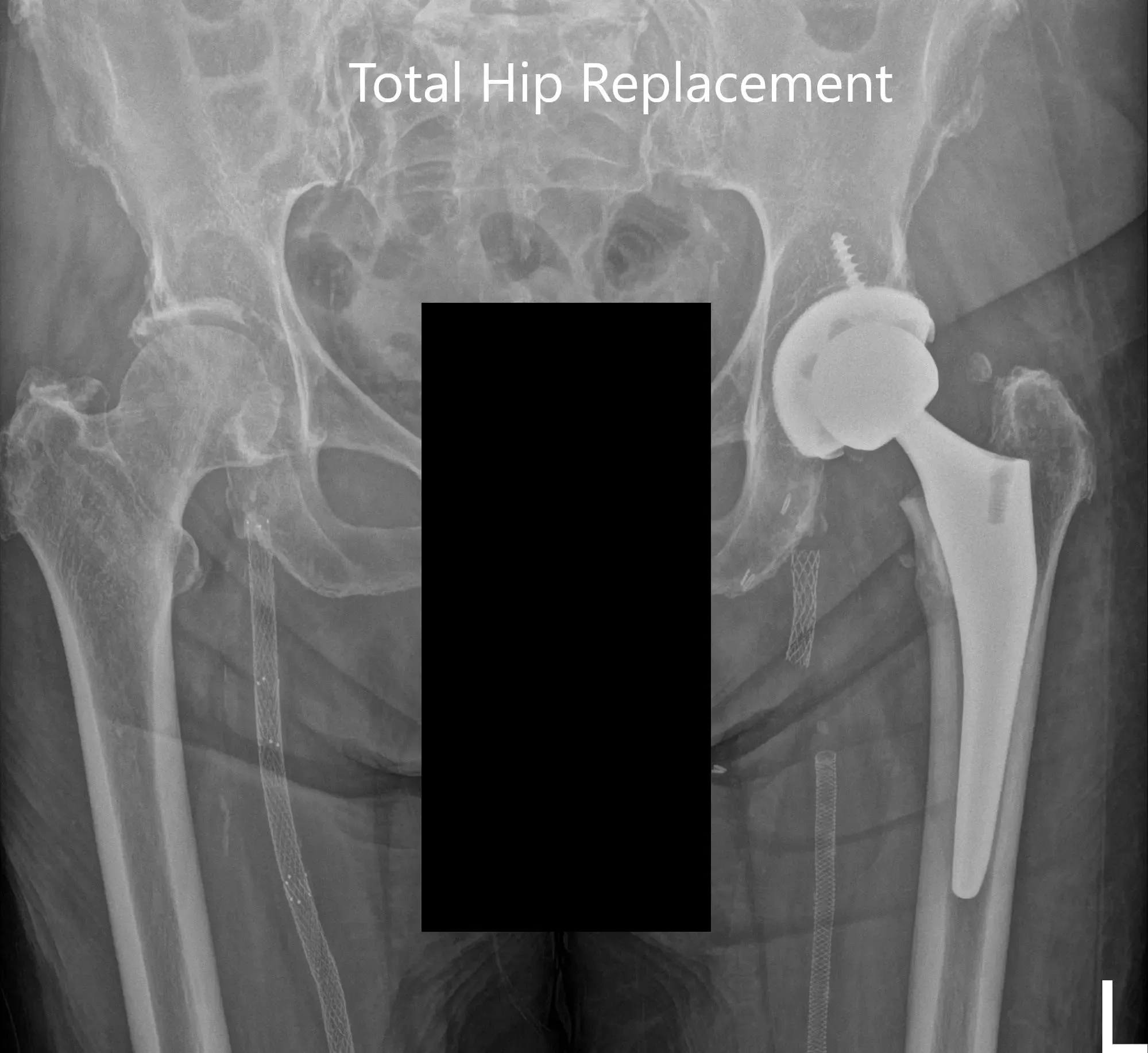
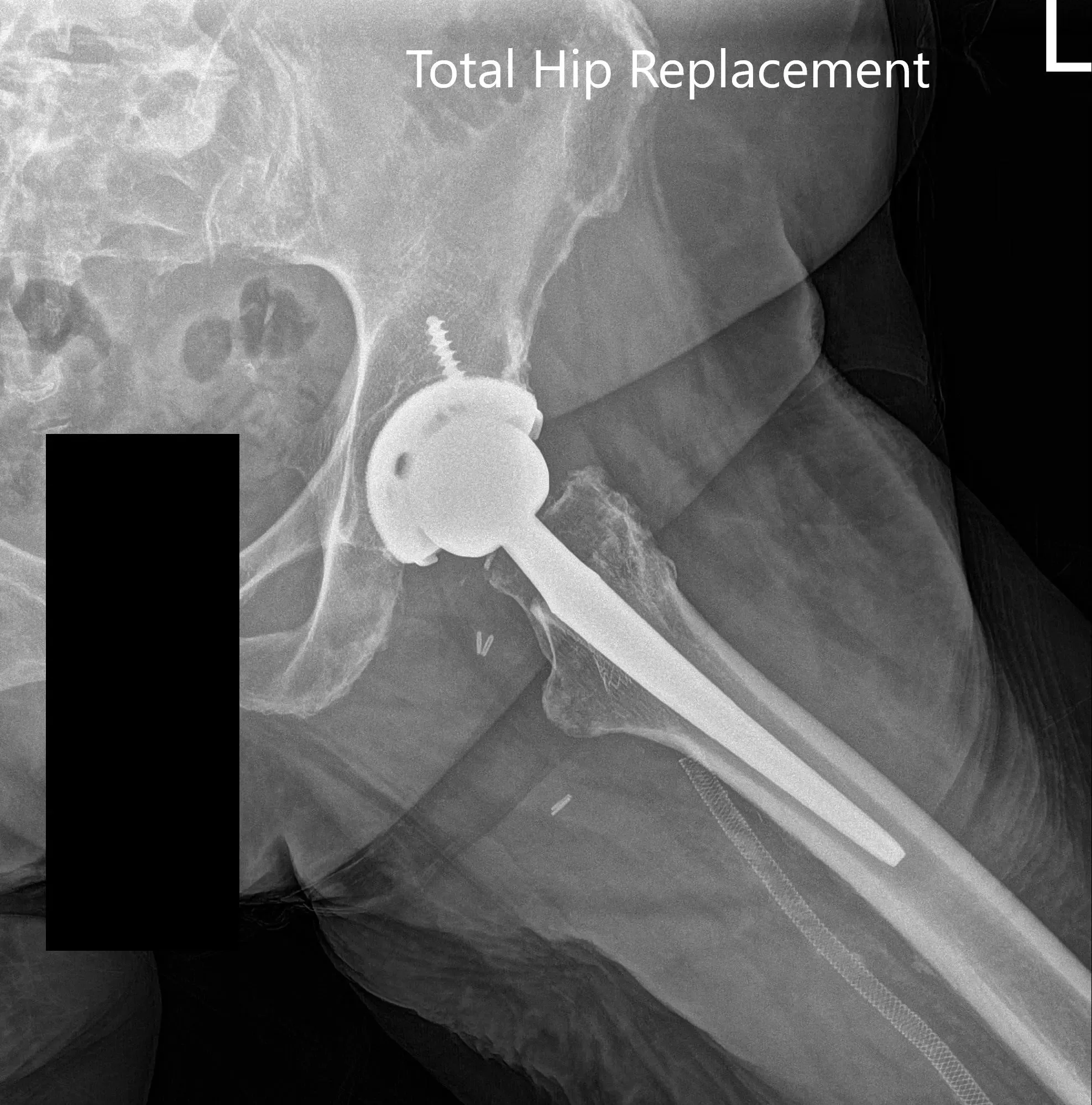
Postoperative X-ray images showing AP and lateral images
The postoperative recovery was excellent with the pain well managed with medications. He was started on aspirin 325mg for deep vein thrombosis prophylaxis. Weight-bearing was allowed as tolerated with support. The patient’s surgical wound staples were removed uneventfully. His physical therapy was focused on gait training, strengthening of muscles and range of motion exercises.
Upon three months follow up, he demonstrated a full range of motion with no pain. He complained of mild stiffness and was advised to continue physical therapy and home exercise program. He was happily back to activities he enjoyed. The increased mobility made him happy and more inclusive in his family.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 11, 2025.
