Some people have arthritis in both hips and need both joints replaced. This can be done in two separate surgeries (staged) or both at once in a single operation. Replacing both hips in one sitting is called a simultaneous bilateral total hip replacement.
It can mean one anesthetic and one recovery, but it is a bigger operation, so it is offered to carefully selected, otherwise healthy patients.
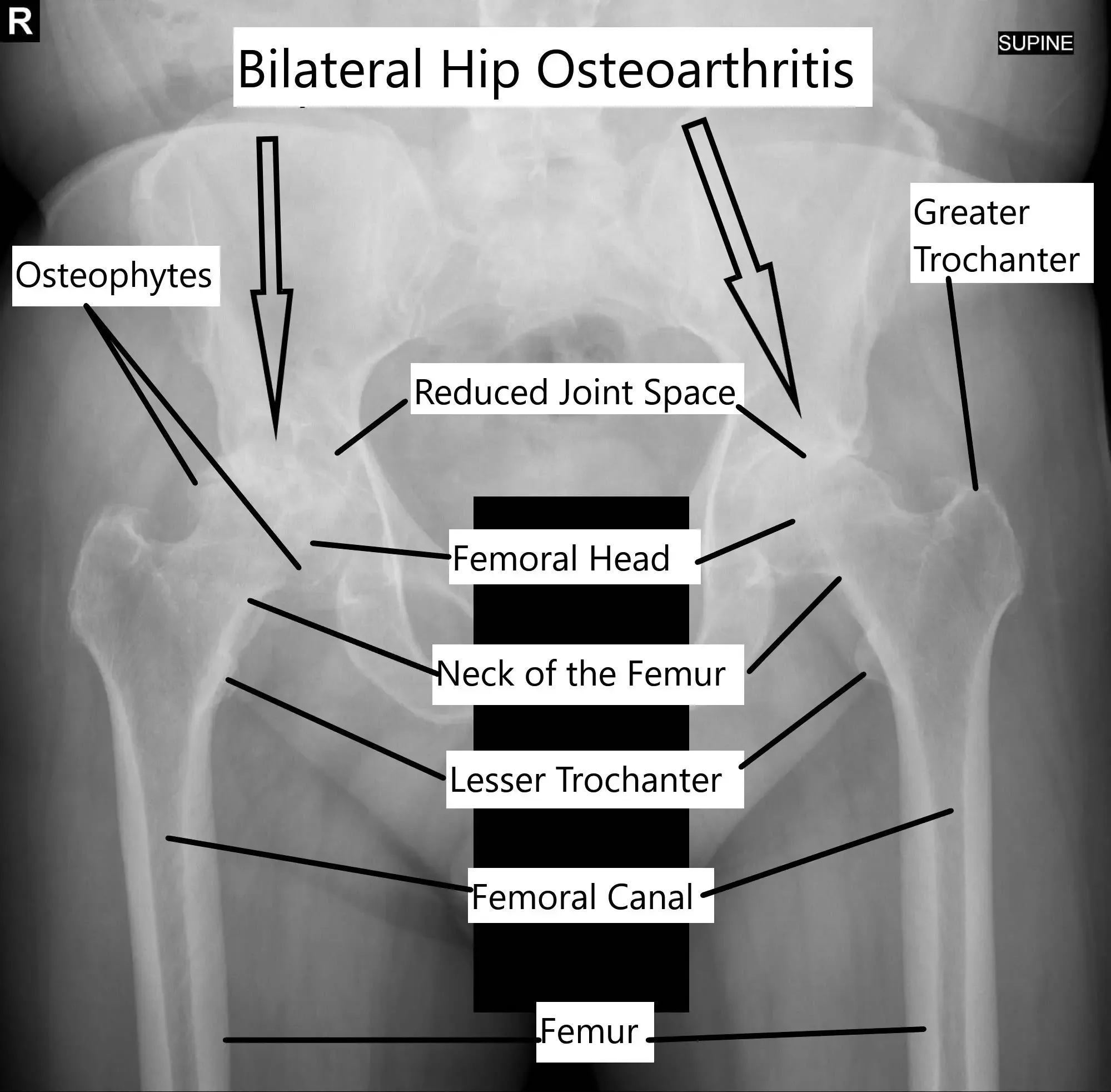
Osteoarthritis of bilateral hip joints.
About bilateral hip arthritis
A total hip replacement treats hip arthritis that no longer responds to non-surgical care like physical therapy, injections, or pain medicine. When arthritis affects both hips, the pain can make everyday things hard: walking, climbing stairs, getting out of a chair, even tying your shoes.
Several conditions can wear out both hips at the same time:
- Osteoarthritis: the smooth cartilage that cushions the joint wears away with age. It often starts in one hip, and the other tends to follow. Injury can also cause it earlier in life (post-traumatic arthritis).
- A hip that did not form properly at birth, which becomes a poor fit over time and wears out early.
- Rheumatoid arthritis: the immune system attacks the joint. It usually affects several joints and commonly involves both hips.
- Avascular necrosis: the bone loses its blood supply and collapses. When it is not caused by injury, it often affects both hips at once.
Candidates for simultaneous bilateral hip replacement
Doing both hips at once is a bigger operation, so patients are chosen carefully and cleared by their primary care doctor first. It tends to suit people who are younger and more active, usually under 70 to 75.
Good candidates have already tried non-surgical treatment, do not have major heart, lung, kidney, or blood-vessel disease, are ideally not significantly overweight, and are motivated to put the work into rehab.
The bilateral hip replacement procedure
Both hips are cleaned and draped at the same time, and the surgeon starts with one hip. The joint can be reached from the back (posterior approach) or the front (anterior approach); the choice depends on your anatomy and your surgeon’s experience. The anterior approach can make positioning the second hip easier.
For each hip, the worn socket is cleared and a new cup (metal alloy or ceramic) is fixed with screws or a tight press-fit. The worn ball at the top of the thigh bone is removed, and a metal stem is set into the bone, held by a press-fit or bone cement. A new ball goes on the stem, and a smooth, durable plastic liner (polyethylene) sits between the ball and cup so the joint glides.
The first incision is closed and the position is checked with a live X-ray (fluoroscopy). The surgeon then repeats the whole process on the second hip.
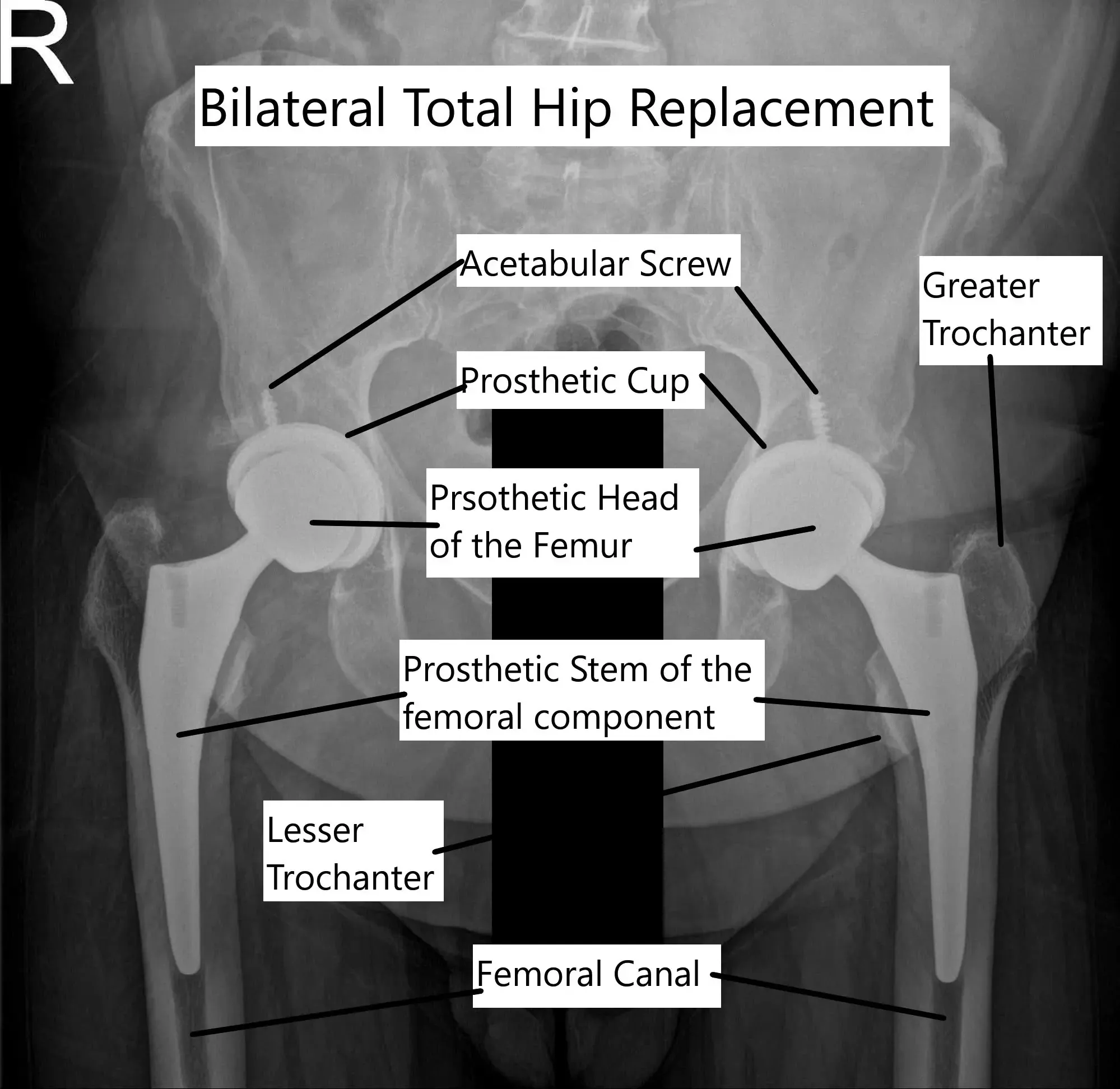
Bilateral total hip replacement.
Benefits of doing both hips at once
For the right patient, replacing both hips in one operation has real advantages:
- One trip to the operating room and one anesthetic, instead of two.
- Less total time off work, since you take time off once rather than twice.
- You rehab both hips together, rather than going through recovery twice.
- It can cost the healthcare system less than two separate surgeries.
Risks of simultaneous bilateral hip replacement
Because it is one larger operation, doing both hips at once carries more risk than a single hip replacement:
- More blood loss, and lower blood counts (hemoglobin) afterward.
- A higher chance of needing a blood transfusion, which carries its own risks.
- A longer operation, often a longer hospital stay, and a greater chance of needing inpatient rehab afterward.
- A higher overall chance of complications such as blood clots in the leg (deep vein thrombosis), a clot that travels to the lungs (pulmonary embolism), or infection.
Simultaneous vs staged hip replacement
The main alternative is a staged replacement: the two hips are done in separate surgeries, usually 3 to 4 months apart. This is the more common approach. It means two anesthetics, two recoveries, and two stretches of time off, but each surgery is smaller and spreads the risk out.
Simultaneous surgery is generally reserved for selected, healthy, motivated patients. The right choice depends on your health, your age, and your goals, and it is a decision to make together with your surgeon.
Cost Information
This procedure using the CPT code 27130 is covered by Medicare and most major insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), as well as most workers’ compensation and no-fault insurance plans. Your out-of-pocket cost depends on your specific plan, deductible, and the medical necessity criteria that apply to your case.
Call our billing team at Complete Orthopedics at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs. For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 24, 2026.

