A 72-year-old female was referred to us for a left hip and thigh pain. The patient had an anterior hip replacement done 2 months ago by an outside physician. The patient stated he experienced acute pain in the left hip and thigh while getting up from the bed. The pain was moderate in intensity and was aggravated on weight-bearing.
The patient was a retired firefighter who underwent total hip replacement for hip arthritis. The patient was apparently well after the primary replacement surgery and was compliant with hip precautions. She was in visible discomfort due to pain and stated she felt her left leg was shorter compared to the right leg.
The patient had a medical history of hypothyroidism, asthma, and dyslipidemia, both conditions currently controlled with medications. She was currently on levothyroxine, albuterol, and atorvastatin. She was a former smoker having quite 20 years ago. Her past surgical history included left shoulder arthroscopic surgery done 6 years ago.
Her physical examination revealed a restricted range of motion about the left hip secondary to pain. She was unable to do a straight leg raise test on the left side. There was tenderness at the left anterior joint line and the rotations were painful. There was no distal neurological deficit.
There was left lower extremity true shortening of 1 cm. She was ambulatory non-weight bearing on the left leg with the help of crutches. The right hip, bilateral knees, bilateral ankles, and lumbosacral spine, both upper extremities were normal on examination.
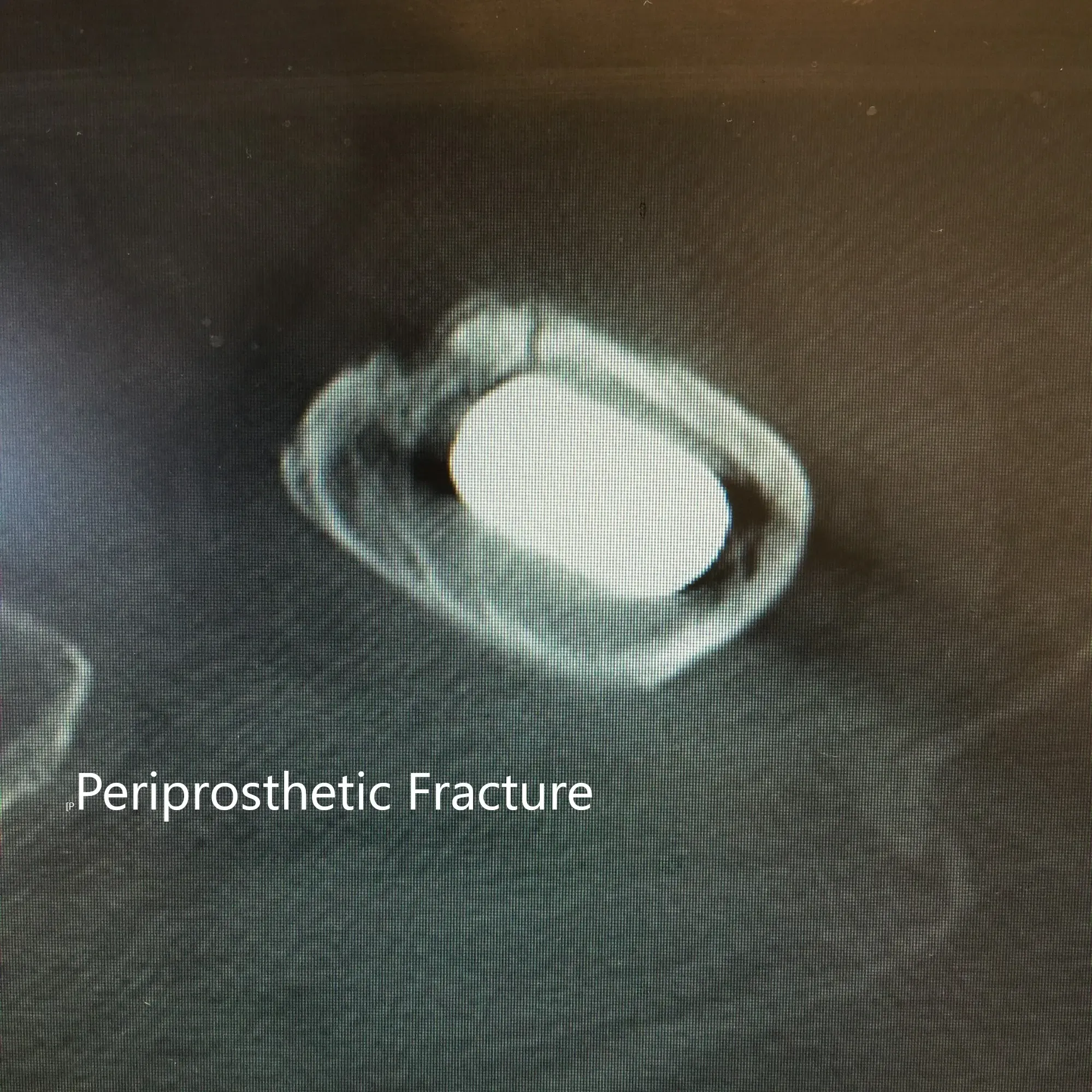
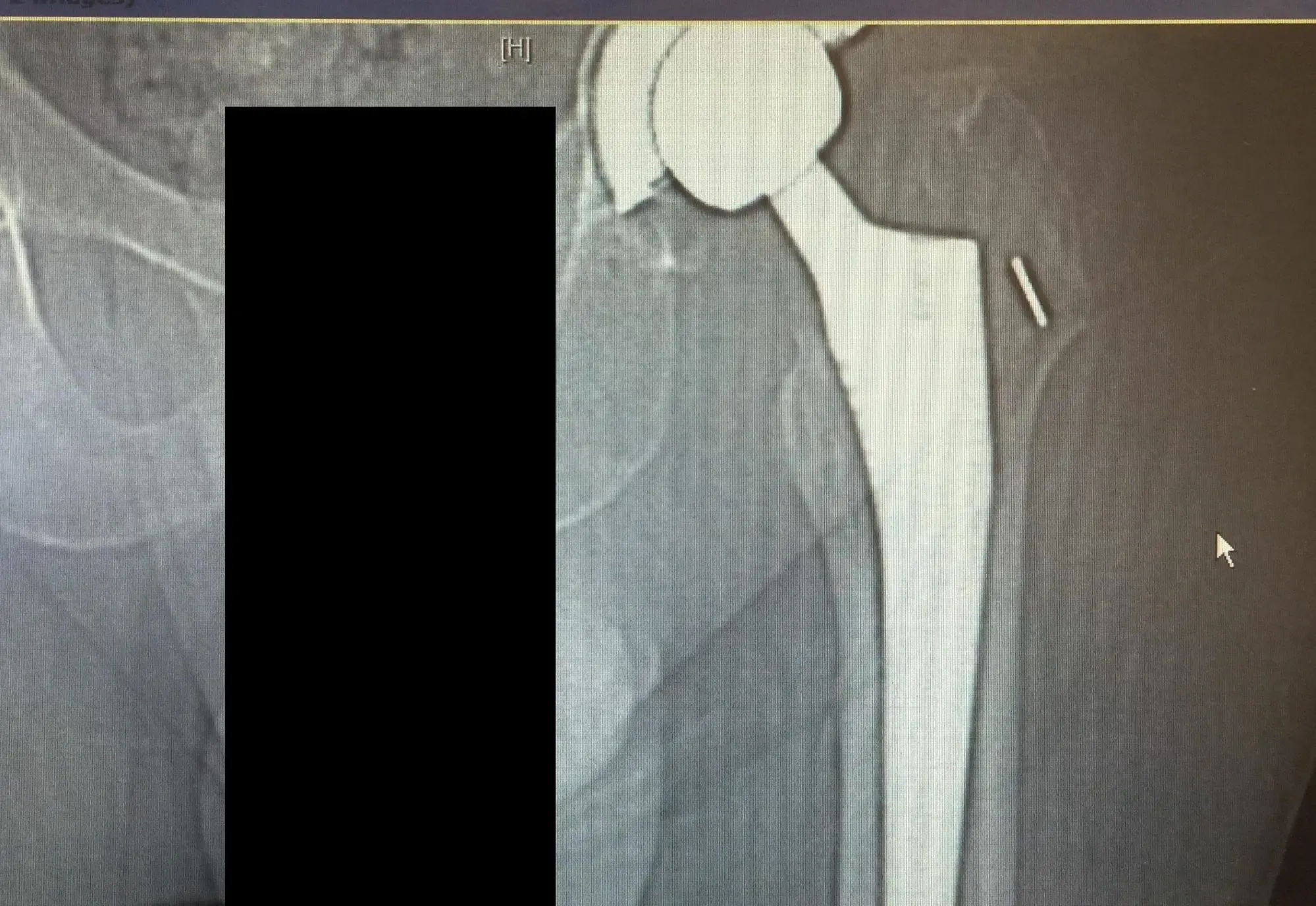
CT scan and X-ray of the left hip revealed a nondisplaced periprosthetic fracture of the proximal femur anteromedially with subsidence of the stem.
After assessment of all her medical conditions and physical examination, she was advised for revision surgery. An open reduction and internal fixation of the fracture with revision of the femoral component was planned. Risks, benefits, and alternatives were discussed at length with her and her family. The patient and her family agreed to the operative plan.
Operative Notes:
Preoperative diagnosis: Left hip periprosthetic fracture with a loose stem and with subsidence.
Procedure:
- Open reduction internal fixation of the left femur with revision of the left femoral component.
- Physician-directed fluoroscopy, less than an hour
The patient was brought to the operating room and anesthesia was obtained by the anesthesiologist. Before bringing the patient in, the family, as well as the patient, understood the increased risk of the revision procedure.
After anesthesia was obtained, the patient was definitively positioned with left hip up in the lateral position and the left hip was then draped and prepped in the usual sterile manner. A curved incision centered over the greater trochanter was used for the arthrotomy. Skin and subcutaneous tissues were incised. The fascia was then divided.
The fracture was then identified. The hip was then placed in internal rotation and the posterior soft tissue structures were then taken down and tagged for future repair. The loose stem was then removed. The fracture was identified again and cables were placed around the fracture. The femur was then reamed.
The final distal femur was then placed into position. The proximal femur was then reamed and the head was then placed into position and the hip was then reduced and intraoperative fluoroscopy picture was then taken. The hip was slightly lengthened and the final distal component was taken out.
The femur was then reamed more and the final component was then placed back into position. The proximal femur was reamed again. The prior head was then placed into position.
The hip was then relocated and trialed through a physiological range of motion and the hip was found to be stable in all physiological ranges of motion. Intraoperative fluoroscopy was obtained additionally.
The hip was dislocated. The trial components were then removed. Thorough lavage was given. The final proximal body was placed into position along with the final head. The hip was then relocated. The cables were then tightened again and crimped. The cables were then cut.
With the hip relocated, thorough lavage was given. Drill holes wem made in the greater trochanter and the posterior soft tissue structures were then tagged to the greater trochanter through transosseous tunnels. Thorough lavage was given.
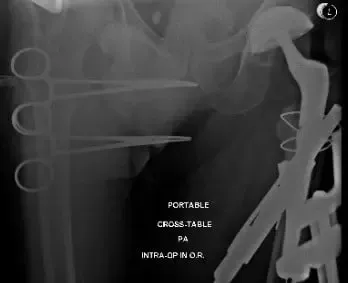
Intraoperative and postoperative X-ray images showing cables used for fracture fixation and revised long femoral stem.
DVT prophylaxis and her pain was well managed with medications. Her surgical wound was inspected to be clean, dry and intact. The skin staples were removed 15 days post-surgery.
She was advised physical therapy and a home exercise program to strengthen her muscles. She was compliant with the hip precautions post-surgery. Weight-bearing was allowed as tolerated. Three months after the surgery she was walking without the support and complained of no pain (0/10). She was doing her physical therapy and had discontinued the aspirin. The patient expressed relief from the success of the surgery and was happy with the outcome.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 9, 2025.
