Leg length discrepancy refers to a difference in the length of the legs following total hip replacement surgery. This condition can occur when one leg feels longer or shorter than the other, either because of an actual difference in bone length or a functional imbalance where the length is perceived differently. Although it can be concerning for patients, this complication is rare and often resolves naturally within a few months after surgery.
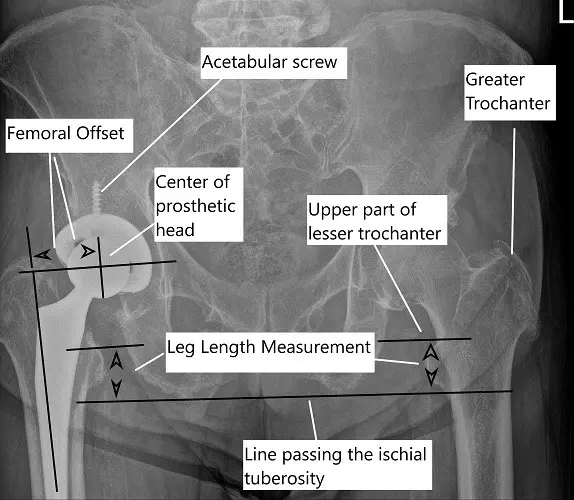
X-ray of the pelvis showing leg length measurement in a post-op total hip replacement of the right hip.
How Common It Is and Who Gets It? (Epidemiology)
Leg length discrepancy after hip replacement is uncommon, thanks to modern surgical techniques and implant designs. When it does occur, it is usually mild and temporary. The condition tends to affect patients recovering from hip arthritis who have pre-existing pelvic tilt or tight muscles around the hip joint. Both men and women can experience this issue, but it is more likely in patients with advanced deformity or prior surgery on the same hip.
Why It Happens – Causes (Etiology and Pathophysiology)
Leg length discrepancy may occur due to several factors during or after surgery:
- Pelvic tilt and muscle tightness: Arthritis causes shortening of the diseased hip, and the body compensates with pelvic tilting. After surgery, the new joint restores normal length, but the tight muscles around the hip may cause the pelvis to remain tilted, making the leg feel longer.
- Surgical technique: Surgeons aim for joint stability and proper alignment. Sometimes, to prevent dislocation, a slightly longer implant or neck may be used, leading to minimal leg lengthening.
- Implant positioning: Malposition of the prosthetic cup or the use of smaller implants in unplanned surgeries can create true shortening.
- Soft tissue balance: Overly tight or lax soft tissues can change leg mechanics and create the perception of uneven length.
How the Body Part Normally Works? (Relevant Anatomy)
The hip joint is a ball-and-socket joint connecting the femoral head (thigh bone) to the acetabulum (hip socket). In a total hip replacement, these structures are replaced with metal and plastic implants designed to restore normal alignment and movement. The surrounding muscles and ligaments provide stability and control. When these soft tissues tighten or relax unevenly, it can alter pelvic balance, leading to the sensation of one leg being longer or shorter.
What You Might Feel – Symptoms (Clinical Presentation)
Patients may notice that one leg feels longer or shorter when standing or walking. They might limp or experience pain in the hip, thigh, or lower back. In true leg lengthening, stretched nerves such as the sciatic or femoral nerve can cause numbness, tingling, or weakness. In true shortening, muscle tension around the hip may be reduced, leading to instability or difficulty balancing. Discomfort typically improves as the body adjusts after surgery.
How Doctors Find the Problem? (Diagnosis and Imaging)
Doctors diagnose leg length discrepancy through a combination of patient history, physical examination, and imaging. The examination includes visual inspection of posture, pelvic alignment, and gait. X-rays are commonly used to measure leg length precisely and determine if the discrepancy is true or functional. CT scans may be ordered in rare cases for more detailed assessment of implant positioning.
Classification
Leg length discrepancy can be classified as:
- True discrepancy: A measurable difference in bone length due to implant positioning or surgical adjustments.
- Functional discrepancy: The legs are equal in length, but muscle tightness or pelvic tilt creates the sensation of unevenness.
Most postoperative discrepancies are functional and improve within a few months.
Other Problems That Can Feel Similar (Differential Diagnosis)
Other conditions that can mimic leg length discrepancy include pelvic obliquity, scoliosis, muscle imbalance, hip or knee contractures, and back problems. Careful examination helps rule out these causes.

Intraoperative image showing loading of the prosthetic acetabular shell.
Treatment Options
Non-Surgical Care – Most cases improve naturally. Physical therapy and stretching exercises help relax tight muscles and correct pelvic tilt. The body often adapts to minor differences (less than 10 mm) without intervention. In some cases, a shoe lift or insert may be recommended for comfort and balance after 6 months.
Surgical Care – Revision hip replacement is rarely required and reserved for severe, persistent discrepancies. Surgery may involve adjusting implant size or position to restore equal leg length.
Recovery and What to Expect After Treatment
Most patients experience gradual improvement in leg length sensation and gait within three to six months. Physical therapy is essential for retraining posture, improving flexibility, and restoring balance. For patients using a shoe lift, comfort typically improves within weeks. True surgical revisions require longer recovery but are uncommon.
Possible Risks or Side Effects (Complications)
Potential complications include persistent pelvic tilt, nerve stretching from lengthening, hip instability from shortening, or continued limp. Lower back pain may develop from altered alignment. However, these risks are rare with proper rehabilitation and monitoring.
Long-Term Outlook (Prognosis)
The outlook for patients with leg length discrepancy after hip replacement is excellent. Most cases resolve without surgery, and long-term function and satisfaction remain high. The advanced precision of modern implants and surgical planning has made significant discrepancies exceedingly rare.
For insurance and cost information, see our Insurance Information page.
Frequently Asked Questions (FAQ)
Q. Is leg length discrepancy after hip replacement permanent?
A. Usually not. Most cases resolve within six months through physical therapy and natural body adaptation.
Q. When should I worry about leg length differences?
A. If the sensation persists beyond six months or causes ongoing pain or limping, consult your orthopedic surgeon.
Q. Can leg length differences be corrected without surgery?
A. Yes. Stretching, physical therapy, and shoe lifts effectively correct most mild discrepancies.
Summary and Takeaway
Leg length discrepancy after total hip replacement is a rare and usually temporary issue. It may result from muscle tightness, pelvic tilt, or surgical adjustments made for stability. Most patients improve with stretching, physical therapy, and time. In very few cases, surgical revision may be considered. With proper care and rehabilitation, patients typically regain balance and comfort within a few months.
Clinical Insight & Recent Findings
After undergoing total hip replacement, some patients may notice a leg length discrepancy (LLD), which can result from several factors such as the surgical technique, preoperative joint deformities, or muscle tightness around the pelvis. A recent study has examined various techniques for reducing LLD after THA, specifically comparing the use of a positioning table with intra-operative radiography, a standard table with radiography, and a standard table without radiography.
Despite the differences in approaches, the study found no significant advantages in controlling LLD with either method. The most important factor was the surgeon’s skill and experience, suggesting that LLD management remains a complex challenge that requires individualized care. (“Study on factors affecting leg length discrepancy after hip replacement – see PubMed.“)
Who Performs This Treatment? (Specialists and Team Involved)
Leg length discrepancy is managed by orthopedic surgeons specializing in hip replacement. The care team may include physical therapists for rehabilitation, radiologists for imaging evaluation, and orthopedic nurses who assist with patient recovery and follow-up.
When to See a Specialist?
If you notice a limp, uneven walking pattern, or persistent pain after hip replacement, you should schedule a follow-up with your orthopedic surgeon. Early evaluation ensures appropriate treatment and faster recovery.
When to Go to the Emergency Room?
Seek emergency care if you experience severe pain, sudden inability to walk, signs of nerve injury such as numbness or weakness, or evidence of hip dislocation following surgery.
What Recovery Really Looks Like?
Recovery typically involves physical therapy, mild soreness during stretching, and gradual improvement in leg balance. Some patients use shoe inserts temporarily. Most resume normal activities comfortably within three to six months.
What Happens If You Ignore It?
Ignoring leg length discrepancy can lead to persistent limping, back pain, or uneven wear on the spine and joints. It may also affect the longevity and stability of the hip implant.
How to Prevent It?
Prevention starts with careful preoperative templating—measuring implant size and placement before surgery. Modern technology such as robotic-assisted surgery and intraoperative imaging further enhances accuracy, minimizing the risk of leg length differences.
Nutrition and Bone or Joint Health
A diet rich in calcium, vitamin D, and protein supports bone healing and joint health after surgery. Maintaining hydration and avoiding smoking or excessive alcohol use promotes better recovery.
Activity and Lifestyle Modifications
Gentle stretching and strengthening exercises help maintain pelvic alignment and prevent stiffness. Patients should gradually resume walking and low-impact activities like swimming or cycling. Good posture and adherence to physical therapy are key for lasting results.
Do you have more questions?
What are the most common symptoms associated with leg length inequality after hip replacement surgery?
Common symptoms include limping, uneven gait, hip or lower back pain, difficulty walking or standing for prolonged periods, and discomfort or instability in the hip joint.
Can leg length inequality affect the stability of the hip joint?
Yes, significant leg length inequality can affect the biomechanics of the hip joint, potentially leading to altered joint loading and stability.
Are there any age-related factors that influence the likelihood of developing leg length inequality after surgery?
Age-related factors such as bone density, tissue elasticity, and healing capacity may influence the development and severity of leg length inequality post-surgery.
How do other pre-existing conditions, such as scoliosis or pelvic tilt, contribute to leg length discrepancy?
Pre-existing conditions like scoliosis or pelvic tilt can affect pelvic alignment and leg length measurement, contributing to leg length inequality.
Is leg length inequality more common in certain types of hip replacement surgeries (e.g., anterior vs. posterior approach)?
Leg length inequality can occur with any hip replacement approach, but its incidence may vary depending on surgical technique, patient anatomy, and surgeon experience.
Can leg length inequality affect the alignment of the spine?
Yes, leg length inequality can lead to compensatory changes in spinal alignment, potentially causing issues such as scoliosis, lordosis, or chronic back pain.
Are there any alternative treatments available for leg length inequality besides surgery and shoe lifts?
Alternative treatments may include physical therapy, corrective exercises, orthotic devices, or specialized footwear designed to improve gait and alignment.
How does leg length inequality impact the distribution of forces across the hip joint?
Leg length inequality can result in uneven weight distribution across the hip joint, potentially leading to increased stress on certain areas and predisposing to joint degeneration or instability.
What are the potential psychological effects of living with leg length inequality?
Living with leg length inequality can cause emotional distress, self-consciousness, and decreased quality of life due to physical limitations, discomfort, and impact on daily activities.
How soon after hip replacement surgery should patients be evaluated for leg length inequality?
Patients should be evaluated for leg length inequality as part of routine postoperative assessment, typically within the first few weeks to months after surgery, depending on individual recovery progress.
Can leg length inequality cause problems with balance and stability?
Yes, leg length inequality can affect balance and stability, potentially increasing the risk of falls, muscle imbalances, and joint strain.
Are there specific exercises or stretches that can help alleviate symptoms of leg length inequality?
Yes, targeted exercises and stretches prescribed by a physical therapist can help improve flexibility, strength, and alignment, reducing symptoms associated with leg length inequality.
What role does physical therapy play in the management of leg length inequality?
Physical therapy plays a crucial role in addressing muscle imbalances, improving joint mobility, optimizing gait mechanics, and enhancing overall functional outcomes in patients with leg length inequality.
How does leg length inequality affect the function of the hip abductor muscles?
Leg length inequality can lead to asymmetrical loading of the hip abductor muscles, potentially causing weakness, fatigue, or compensatory muscle recruitment patterns.
Are there any differences in the rehabilitation process for patients with leg length inequality compared to those without?
Rehabilitation protocols may be tailored to address specific functional deficits and biomechanical issues associated with leg length inequality, focusing on symmetry restoration, gait training, and strength conditioning.
Can leg length inequality affect the success of physical therapy after hip replacement surgery?
Yes, leg length inequality can impact the effectiveness of physical therapy by influencing joint mechanics, muscle function, and overall functional capacity, potentially affecting rehabilitation outcomes.
How does leg length inequality impact the biomechanics of the lower extremities during walking and running?
Leg length inequality can disrupt normal biomechanics, leading to altered gait patterns, increased joint loading, and compensatory movements that may predispose to musculoskeletal injuries or discomfort.
Are there any dietary or lifestyle factors that can influence the risk of developing leg length inequality?
Can leg length inequality affect the outcomes of other orthopedic procedures, such as knee replacement surgery?
Can leg length inequality affect the outcomes of other orthopedic procedures, such as knee replacement surgery?
Yes, leg length inequality can impact the outcomes of other orthopedic procedures by affecting joint mechanics, limb alignment, and overall functional symmetry, potentially influencing patient satisfaction and recovery.
How does leg length inequality affect the alignment of the knees and ankles?
Leg length inequality can alter lower limb alignment, potentially leading to issues such as knee valgus or varus, ankle pronation or supination, and compensatory changes in foot posture.
Are there any specific complications associated with leg length correction surgery?
Complications of leg length correction surgery may include infection, implant failure, nerve injury, nonunion or malunion of bone segments, and recurrence of leg length discrepancy.
How does leg length inequality affect the distribution of pressure on the hip joint during weight-bearing activities?
Leg length inequality can lead to unequal loading of the hip joint during weight-bearing activities, potentially causing abnormal wear and tear, cartilage damage, or predisposing to degenerative joint disease.
Can leg length inequality lead to chronic inflammation or arthritis in the hip joint?
Yes, chronic leg length inequality may contribute to increased stress on the hip joint, leading to inflammation, cartilage degeneration, osteoarthritis, or other degenerative changes over time.
How do surgeons determine the optimal amount of correction needed for leg length inequality during surgery?
Surgeons typically assess leg length inequality preoperatively using clinical examination, imaging studies, and functional assessment, aiming to achieve optimal limb symmetry and functional outcomes based on individual patient factors and goals of treatment.
What are the potential effects of leg length inequality on posture and body mechanics?
Leg length inequality can affect posture by causing pelvic tilt, spinal curvature, or compensatory changes in limb alignment, potentially leading to muscle imbalances, joint strain, and postural dysfunction.
How does leg length inequality impact the biomechanics of the lower extremities during walking and running?
Leg length inequality can disrupt normal biomechanics, leading to altered gait patterns, increased joint loading, and compensatory movements that may predispose to musculoskeletal injuries or discomfort.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on May 15, 2026.
