A 49 year-old lady who grew up in another country and moved to North America several years ago. She had suffered from mild hip discomfort for many years and had a procedure performed on her left hip in her native Iran, the nature of which was not known.
She had never sought further medical attention for it as she found it tolerable. After her move, her hips began to bother her more and more, particularly her left hip which would, at times, prevent her from walking without a gait aid.
She presented to our clinic with progressively debilitating left hip pain that was not responding to analgesic medications or NSAIDs. Use of a cane did help her to ambulate, but did not improve her pain. Her medical history was unremarkable, she had no known medication allergies and only took a regular medication for anxiety. She is a non-smoker.
Physical examination revealed severe pain on attempting to passively range the hip, with active range of motion restricted by pain also. She did have an apparent leg length discrepancy. Examination of the knee was unremarkable.
Plain film radiographs revealed a significantly arthritic hip with dysplastic features on both sides of the joint. Her contralateral hip revealed similar findings, but of lesser severity.
After counselling the patient regarding treatment options, she elected to proceed with hip replacement surgery.
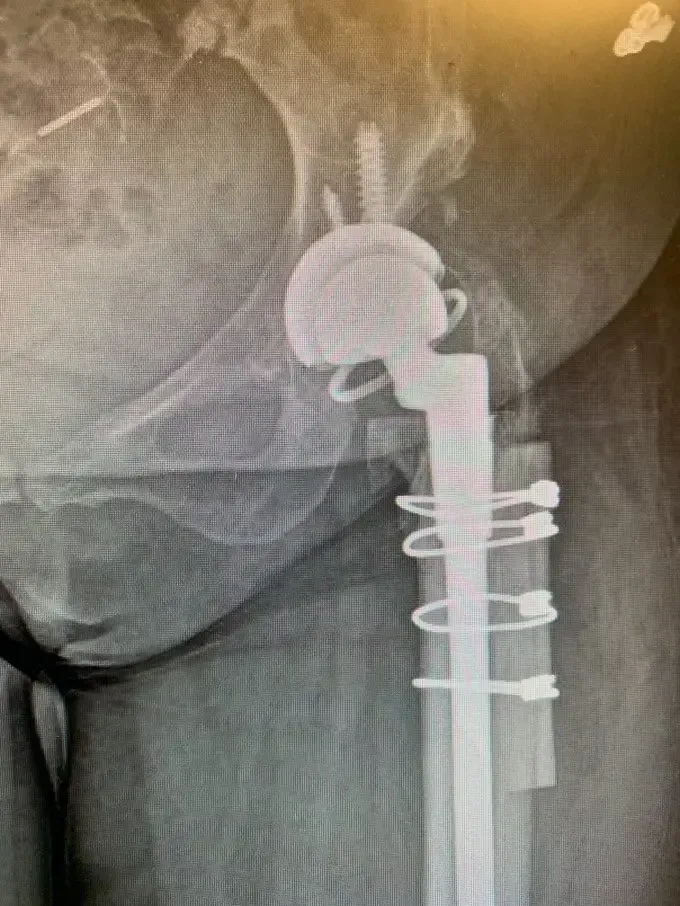
A lateral approach to the hip was used, and despite the patients’ abnormal anatomy, exposure of the hip was gained and the broad, shallow acetabulum was identified. The true acetabulum was identified, and the acetabular component was reamed for and placed without event, augmenting fixation with screws.
Accessing the femoral canal proved challenging, the femoral component was prepared. A femoral shortening osteotomy was then performed removing a significant amount of bone to allow for the hip to be relocated without excessive force.
Once this was completed, the definitive femoral component was placed, the osteotomy was fixed and held together with the removed bone acting as autologous bone graft and the hip was relocated.
6 months on from the surgery, Mrs. M is ambulating well with her pain vastly improved and no longer requiring a cane to walk comfortably. She is under routine surveillance until such time as she wishes to pursue surgical management of her contralateral hip.