Avascular necrosis of the head of the femur is a debilitating disease that affects middle-aged and young adults. The disease is also known as osteonecrosis and may progress rapidly to cause hip pain, deformity, and limp. The management of late-stage avascular necrosis is joint replacement surgery.
In younger patients with early stages of avascular necrosis, head-saving procedures such as vascularized bone grafting may be done. The procedure is mainly done to delay the need for joint replacement surgery, however, with the advancement of implant technology and design, hip replacement surgeries offer excellent results even in young patients.

MRI in the coronal section showing avascular necrosis lesions in both hips
Avascular necrosis occurs as a result of bone death in the head of the femur. Bone death occurs due to disruption of the blood supply of the head of the femur. The disruption of the blood supply may occur as a result of direct trauma to the hip. Traumatic hip dislocations and fractures are commonly associated with avascular necrosis of the hip joint.
Long-term use of corticosteroids for medical diseases such as nephrotic syndrome, rheumatoid arthritis, etc, or secondary to abuse in athletes may lead to avascular necrosis. Avascular necrosis may also occur in patients with a history of alcohol abuse.
In the initial stages of avascular necrosis, there may not be any symptoms and the disease may only be diagnosed on a bone scan or an MRI. With the advancement of the disease, the patient may complain of groin pain that occurs on activity and as well on rest.
During the early stages before the collapse of the head of the femur, attempts are made to preserve the head of the femur. The preservation is aimed to decrease the pressure inside the head of the femur, revitalize the blood supply of the necrotic area, and prevent the collapse of the head of the femur.
The head preservation surgeries include core decompression, stem cell implantation, and bone grafts. With core decompression, the physician tries to reduce the pressure inside the head of the femur and prevent further advancement of the disease. Stem cell therapy in the form of bone marrow graft is done to possibly revitalize the blood supply.
Strut bone grafts such as fibular bone grafts provide not only graft material but also provide structural support to the head of the femur to prevent collapse. Vascularized fibular grafts additionally provide nutrients to the bone graft and are hypothesized to replace the necrotic bone with new bone through creeping substitution.
The fibula is the smaller of the two bones in the leg of the human. The fibula is present on the outer side of the leg. The graft is taken from the middle of the fibula leaving an adequate amount of bone at both ends to continue to provide structural support to the joints of the leg.
The surgeon harvests the graft along with the blood vessels of the bone. The surgeon then passes a wire from the side of the hip joint and serially reams the neck and head of the femur without breaching the subchondral region. The reaming helps to reduce the pressure inside the head of the femur.
The fibular graft is then passed inside the track formed inside the head and neck. A microsurgery technique is then used to attach the graft blood vessels to nearby blood vessels. The blood supply to the graft not only helps to maintain the graft integrity but also brings in bone cells that may slowly replace the dead bone in the head of the femur with new bone.
After the surgery, the patient is advised to follow precautions to protect the graft and to start physiotherapy to aid in early return back to daily activities. At 6 weeks the patients may start protected weight-bearing and slowly progress to complete weight-bearing.
The surgery although aims to preserve the head of the femur, avascular necrosis may still progress. The fibular graft surgery potentially however delays the need for joint replacement surgery. However, with improved techniques and outcomes, joint replacement surgery may be indicated even in young patients.
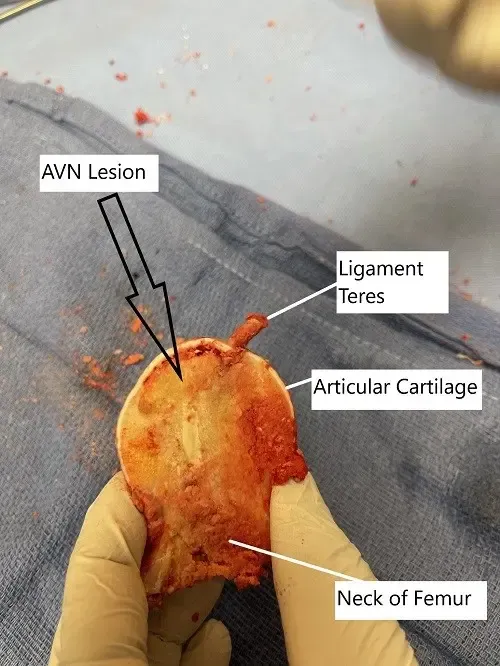
Removed head of femur during surgery showing avascular necrotic lesion
The joint replacement surgery alleviates the pain and deformity associated with avascular necrosis. Modern implants last on an average of 20 years or more and patients who may need eventual arthroplasty after vascularized bone graft are better suited for a primary arthroplasty.
Do you have more questions?
How does the experience and expertise of the surgeon impact the outcomes of fibular bone graft surgery for avascular necrosis of the hip?
The experience and expertise of the surgeon play a crucial role in the outcomes of fibular bone graft surgery for avascular necrosis of the hip, with skilled surgeons often achieving better results in terms of graft integration, joint preservation, and patient satisfaction.
Can fibular bone graft surgery be performed using minimally invasive techniques, and what are the potential benefits of such approaches?
Yes, fibular bone graft surgery can be performed using minimally invasive techniques, which may offer advantages such as smaller incisions, reduced blood loss, faster recovery times, and less postoperative pain compared to traditional open surgery.
How does the age of the patient impact the decision-making process for fibular bone graft surgery for avascular necrosis of the hip?
The age of the patient is an important consideration in the decision-making process for fibular bone graft surgery for avascular necrosis of the hip, with younger patients often being more suitable candidates due to their potential for better bone healing and longer-term outcomes.
Can fibular bone graft surgery be performed in patients with bilateral avascular necrosis of the hip, and if so, what are the potential challenges or considerations?
Fibular bone graft surgery can be performed in patients with bilateral avascular necrosis of the hip, but it may pose additional challenges such as longer recovery times, increased risk of complications, and the need for staged procedures to address both hips.
How does the success rate of fibular bone graft surgery for avascular necrosis of the hip compare to other treatment options available?
The success rate of fibular bone graft surgery for avascular necrosis of the hip varies depending on factors such as disease severity, patient characteristics, and surgical technique. Comparative studies may help determine the effectiveness of fibular bone graft surgery relative to other treatment modalities.
Are there any long-term complications or considerations associated with fibular bone graft surgery for avascular necrosis of the hip that patients should be aware of?
Long-term complications of fibular bone graft surgery for avascular necrosis of the hip may include graft failure, nonunion, arthritis, or progression of avascular necrosis in other areas of the hip joint. Regular follow-up with a healthcare provider is essential to monitor for potential complications.
How does the location and size of the avascular necrosis lesion in the hip joint influence the decision to perform fibular bone graft surgery?
The location and size of the avascular necrosis lesion in the hip joint may influence the decision to perform fibular bone graft surgery, with larger or more centrally located lesions often warranting more extensive surgical intervention.
What imaging studies are used to assess the success of fibular bone graft surgery for avascular necrosis of the hip, and how often are they performed postoperatively?
Imaging studies such as X-rays, MRI, or CT scans may be used to assess the success of fibular bone graft surgery for avascular necrosis of the hip, with follow-up intervals determined by the surgeon based on individual patient factors and disease progression.
Are there any lifestyle modifications or precautions recommended after fibular bone graft surgery for avascular necrosis of the hip to prevent disease recurrence?
Yes, lifestyle modifications such as avoiding excessive weight-bearing activities, quitting smoking, moderating alcohol intake, and maintaining a healthy lifestyle may help reduce the risk of disease recurrence after fibular bone graft surgery for avascular necrosis of the hip.
What are the criteria used to determine if a patient is a suitable candidate for fibular bone graft surgery for avascular necrosis of the hip?
Candidates for fibular bone graft surgery for avascular necrosis of the hip are typically those with early to moderate-stage disease, intact joint integrity, and adequate bone stock to support the graft.
Can fibular bone graft surgery prevent further progression of avascular necrosis in the hip joint, or is it primarily aimed at relieving symptoms?
Fibular bone graft surgery aims to provide structural support to the hip joint, potentially preventing further collapse and preserving joint function. However, its ability to halt the progression of avascular necrosis depends on various factors and may not always be guaranteed.
How long does it typically take to recover from fibular bone graft surgery for avascular necrosis of the hip, and what is the rehabilitation process like?
Recovery from fibular bone graft surgery for avascular necrosis of the hip may take several months to a year, with initial weight-bearing restrictions followed by gradual rehabilitation exercises to restore strength, range of motion, and function.
Are there alternative treatments to fibular bone graft surgery for avascular necrosis of the hip, and how do they compare in terms of effectiveness?
Yes, alternative treatments for avascular necrosis of the hip include core decompression, vascularized bone grafting, osteotomy, and total hip replacement. The choice of treatment depends on factors such as disease severity, patient age, and surgeon preference.
How successful is fibular bone graft surgery in treating avascular necrosis of the hip, and what factors contribute to its success?
The success of fibular bone graft surgery in treating avascular necrosis of the hip depends on various factors, including the stage of the disease, the quality of the graft, surgical technique, patient factors, and postoperative rehabilitation.
Can fibular bone graft surgery be performed as a standalone procedure for avascular necrosis of the hip, or is it often combined with other treatments?
Fibular bone graft surgery can be performed as a standalone procedure for avascular necrosis of the hip, but it may also be combined with other treatments such as core decompression or total hip replacement, depending on the extent and severity of the disease.
How long does it take for a fibular bone graft to integrate and provide structural support in the hip joint?
The timeline for integration of a fibular bone graft into the hip joint varies but typically ranges from several months to a year, during which the graft gradually incorporates with the surrounding bone tissue.
What are the limitations or potential risks of fibular bone graft surgery for avascular necrosis of the hip?
Like any surgical procedure, fibular bone graft surgery for avascular necrosis of the hip carries potential risks such as infection, blood loss, nerve injury, and failure of the graft to integrate properly with the host bone.
Are there different stages of avascular necrosis, and how do they affect treatment options?
Yes, avascular necrosis progresses through stages ranging from early changes in blood supply to advanced collapse of the bone. Treatment options may vary depending on the stage of the disease.
How does avascular necrosis affect the blood supply to the hip joint?
Avascular necrosis disrupts the blood supply to the hip joint, leading to inadequate oxygen and nutrients reaching the bone tissue, which ultimately results in bone cell death and tissue damage.
What is the typical progression of avascular necrosis if left untreated?
If left untreated, avascular necrosis of the hip can progress through stages characterized by increasing bone damage, collapse of the femoral head, degenerative changes in the hip joint, and eventual joint dysfunction.
Can avascular necrosis of the hip progress without treatment?
Yes, avascular necrosis of the hip can progress without treatment, potentially leading to further bone damage, collapse of the hip joint, and severe pain or disability.
Are there any risk factors associated with avascular necrosis of the hip?
Yes, several risk factors can predispose individuals to avascular necrosis of the hip, including trauma, corticosteroid use, excessive alcohol consumption, certain medical conditions like sickle cell disease, and joint diseases such as rheumatoid arthritis.
How common is avascular necrosis of the hip?
Avascular necrosis of the hip can occur in various conditions but is relatively rare. It may affect individuals of any age but is more commonly seen in middle-aged adults.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on March 4, 2026.
