A retired businessman presented to our office with complaints of bilateral groin pain. The patients first noticed the pain four years ago but didn’t recall any inciting event. The pain was moderate initially but had significantly increased in intensity for the past one month.
The patient experienced constant pain which was exacerbated on activities such as prolonged standing, walking, getting up from a chair or navigating stairs. He was unable to bend or even perform his daily activities such as getting up from a toilet seat. He had earlier tried pain medications but the relief was only temporary.
He went to different physicians who told him he had idiopathic avascular necrosis of both hips. He was prescribed bisphosphonates, cholesterol-lowering medications, and blood thinners in an attempt to slow the progression.
He was active physically before the onset of the disease process and was dismayed at his lack of activity secondary to pain. The pain was described as a dull ache that would turn to sharp pain on activity. There was no radiation of the pain.
He was a former smoker and social drinker. His past medical history was positive for hyperlipidemia, high blood pressure, and asthma. He denied any intake of steroids or any illicit drugs. His past surgical history was positive for an anterior cervical decompression and fusion surgery fifteen years ago. He denied any past history of trauma or surgery around the hips.
On physical examination, his gait was steady and coordinated. The bilateral shoulders, anterior superior iliac spines, patella, and malleolus were at the same level. There was no wasting of the gluteal muscles and the thighs. There was no functional or structural scoliosis of the spine. The lumbar lordosis was not exaggerated.
On the supine examination, both the anterior superior iliac spines were at the same level. There was no leg length discrepancy. The skin on both the groins was normal. There was no local rise in temperature or any swelling. Tenderness was present on deep palpation of the bilateral anterior joint line.
The bilateral hip range of motion was moderately restricted in internal rotation and abduction. The rotational movements were particularly painful but there was an absence of any fixed deformity. The differential rotation was present in hip flexion in both the hips.
The power, bulk, and tone of bilateral lower extremities were normal. The examination of the lumbar spine, bilateral knee and ankles were normal. The peripheral pulses were palpable and comparable bilaterally.
Imaging studies in the form of an X-Ray was obtained which suggested sclerosis of the bilateral head of the femur with acetabulum changes. An MRI was obtained which suggested avascular necrosis of both hips.

Preoperative X-ray of the pelvis with both hips in the frog-legged lateral view showing AVN of the bilateral hips.

Preoperative X-ray of the pelvis with both hips in anteroposterior view showing AVN of the bilateral hips.
The left femoral head was collapsed with irregular contour and shows areas of altered signal intensity with a line of demarcation. Hypointense areas both on T1WI & T2WI seen in head suggestive of sclerosis. Surrounding marrow edema seen. A small amount of joint effusion with few osteophytes seen. The joint space was preserved.
The right femoral head shows areas of altered signal intensity with serpiginous demarcation line visualized, Hypointense areas both on T1WI & T2WI seen in head suggestive of sclerosis. The femoral head contour was normal. Surrounding marrow edema is seen. Small joint effusion is seen. Joint space is preserved.
Percentage necrotic areas in bilateral femoral heads are approximately 60-70 %.

T1WI coronal section of MRI showing AVN hip.

T2WI coronal section of MRI showing AVN hip.

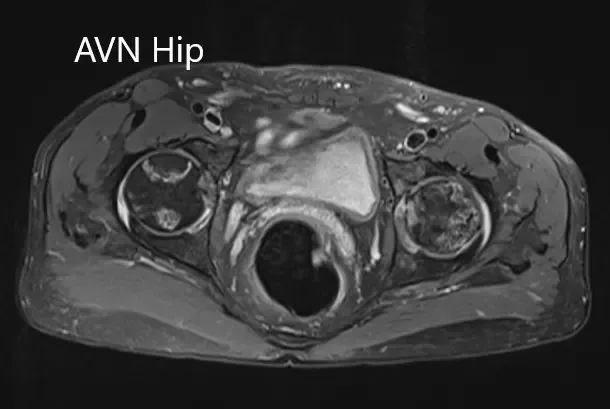
Axial sections of the T1WI and T2WI of MRI.
Considering the lifestyle limiting bilateral hip pain, the patient was advised bilateral total hip replacement. Risks, benefits, and alternatives were discussed at length with the patient. The patients agreed with the plan.
The patient underwent a bilateral total hip replacement. There was no distal neurological deficit post-op. The vitals of the patient remained stable post-op. Pain medications were given to manage postoperative pain. Aspirin was started to prevent deep vein thrombosis.
The patient was allowed to bear weight as tolerated and walked with support. He was compliant with hip precautions and physical therapy. Three months post-op, he was walking without any support and completely pain-free. The patient had an excellent range of motion.
He was back to his baseline activities and was able to walk, climb stairs, drive his car and do daily activities without any limitation. He was delighted at the outcome of the procedure.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 9, 2025.
