A 65-year-old female presented to our office for a second opinion regarding her worsening right knee pain. She previously had a left knee total replacement from an outside physician 2 years back. The patient stated she had tried nonsurgical treatment options with no relief. She reported the pain to be constant since the past 5 months interfering with her sleep.
She first noticed the pain in her left knee about 5 years ago. The right knee also started bothering her subsequently. Conservative management in the form of cortisone injections and physical therapy helped ease her right knee pain. The left knee was treated with surgical management in the form of knee replacement.
Recently, the right knee started getting worse since the problem started. The pain was described as a dull ache to sharp in character located diffusely in the right knee. The intensity was moderate to severe occurring constantly. Activities such as bending, kneeling, using stairs, walking, standing, twisting, squatting made the pain worse.
She was an avid fitness enthusiast regularly doing yoga and enjoyed fencing on the weekend. However, recently she was spending much of her time at home resting. She stated any form of activity made her apprehensive about precipitating the pain. She described the pain to be constant.
She was a nonsmoker and denied any known drug allergies. She denied any form of past medical history and her only surgical history was positive for the left knee arthroplasty. She lived with her husband and was currently working as a yoga instructor.
Physical examination revealed mild swelling in her right knee. The overlying skin was normal with no scar, sinus or erythema. There was no local rise of temperature over the knee. There was mild genu varum deformity. The gait of the patient was antalgic with a reduced stance phase on the right side.
There range of motion on the right side was 5 – 80 degrees and a full range of motion on the left side. The bulk of the muscles was normal with full strength. There was no sign of any instability in the coronal, sagittal and axial plane. The examination of the right knee revealed a linear scar present anteriorly consistent with previous surgery.
The examination of the bilateral hip and knee was normal. There was an absence of any neurological deficit. Bilateral lower extremity pulses were palpable and good volume. Imaging studies revealed severe tricompartmental right knee osteoarthritis.
In view of lifestyle limiting osteoarthritis of the right knee, the patient was advised custom total knee replacement. The patient had exhausted all conservative options and wanted to get back to her baseline routine as soon as possible. She agreed with the plan and went ahead for the operation.


Preoperative topography CT scan images of the lower extremities.
A preoperative CT scan was obtained a few weeks prior to the procedure. Detailed models of the patient’s anatomy were constructed. Accurate bone cuts and offsets were determined to preplan the surgery. Disposable unique jigs and customized implants were made to match the patient’s anatomy.
OPERATION: Right total knee arthroplasty
IMPLANTS USED: Custom femoral implant with a 6 mm polyethylene inserts with a custom tibial implant with a patella of size 38 mm, 8.5 mm.
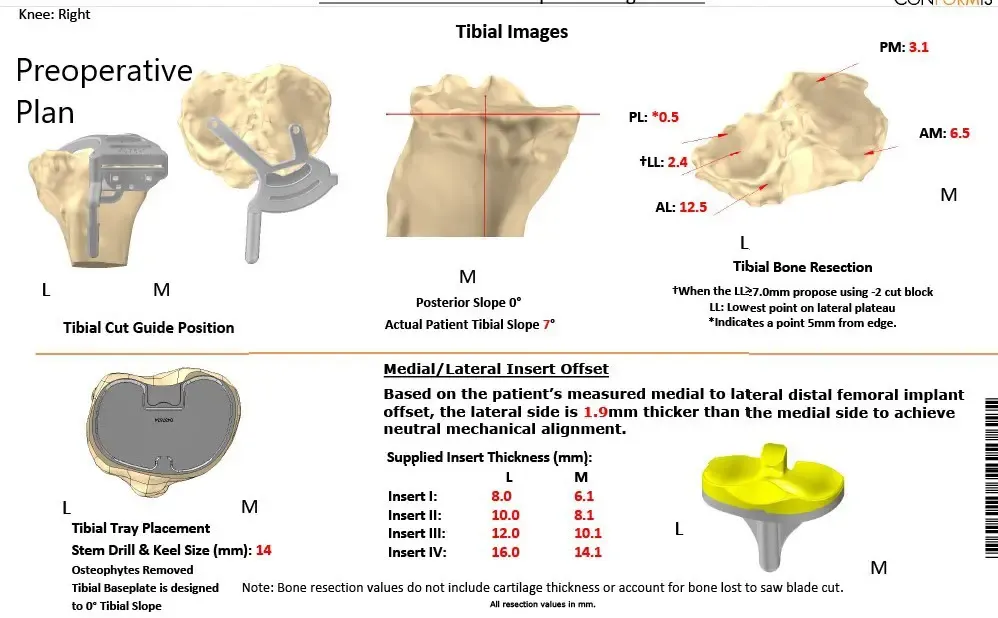
Complete Orthopedics patient-specific surgical plan for a customized right knee replacement in a 65-year-old female.
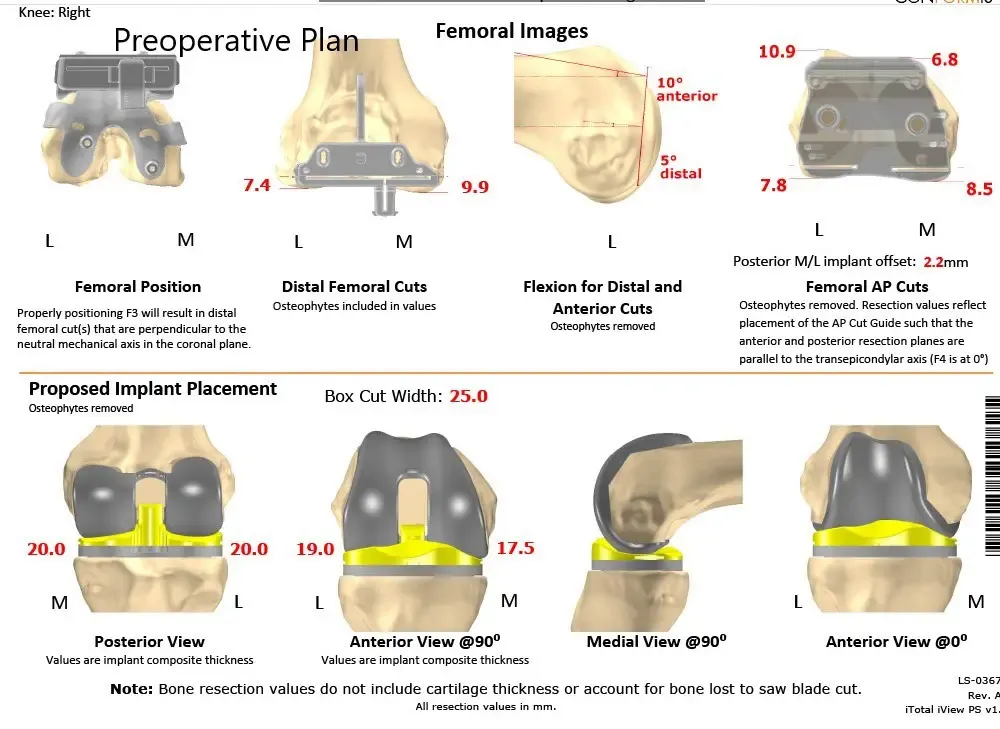
Complete Orthopedics patient-specific surgical plan for a customized right knee replacement in a 65-year-old female (scan 2)
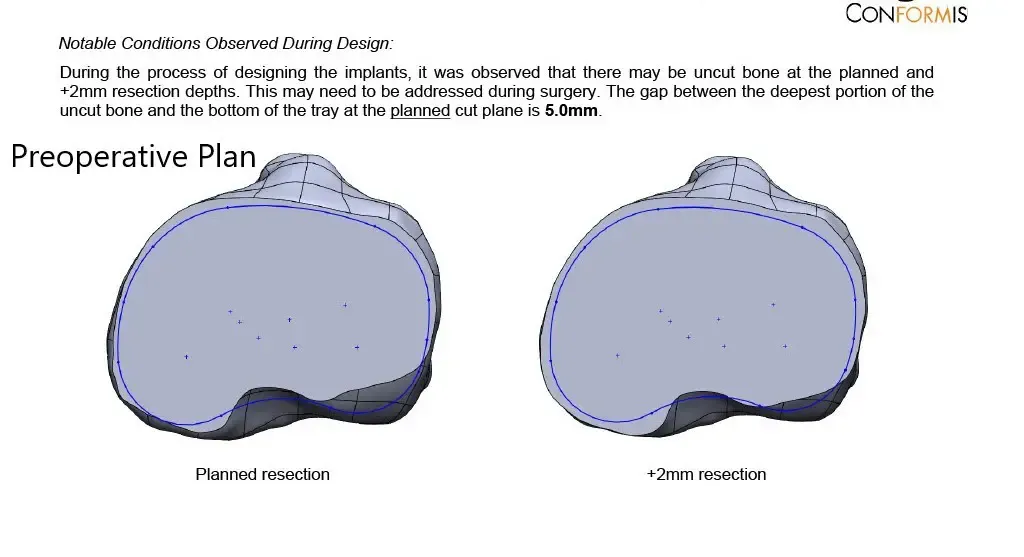
Complete Orthopedics patient-specific surgical plan for a customized right knee replacement in a 65-year-old female (scan 3)

DESCRIPTION OF PROCEDURE: The patient was brought to the operating room after obtaining informed consent and signing the correct surgical site. The risks, benefits, and alternatives were discussed with him at length.
The patient understands that he is at increased risk of complications. The patient was definitively positioned. Tourniquet was placed over the right thigh.
Right lower extremity was draped and prepped in the usual sterile manner. The patient was draped and prepped in the usual sterile manner. A straight incision was used for the arthrotomy. Ski and subcutaneous tissues were incised. Medial parapatellar arthrotomy was performed.
The tibia was exposed. Custom tibial guides were used to make the tibial resection. The tibial resection was checked and was found to be correct.
Attention was then turned towards the femur. Custom jigs were used for distal and chamfer resections. The box cut was then made.
Medial and lateral laminar spreaders were used for resecting the remainder of the meniscus and the cruciate. The knee was then collapsed, and the patellar resection was performed.
Drill holes were made in the patella. The patellar osteophytes were then resected. Gap balancing was performed and was found to be correct. Resections were checked and were found to be correct.
The tibial preparation was then made. The trial femur was then placed into position, followed by the trial tibia, followed by the trial poly. The knee was then ranged to a full range of motion, and the patellar tracking was found to be correct. Full-extension was obtained and full flexion of the knee was obtained. The knee was stable in all range of motion.
Trial components were then removed. The injection was given. The femur was cemented into position. Excess cement was removed. The tibia was cemented into position. Excess cement was removed. Poly was then placed into position, and the knee was then reduced and held in full extension with a bump under the ankle.
The patella was then cemented into position, and excess cement was removed. The patellar compression was achieved with a patellar clamp. After the cement hardened, the patellar clamp was removed. Thorough lavage was given. Medial parapatellar arthrotomy was closed with 0 Vicryl and with Stratafix. Cutaneous tissues were closed with O Vicryl. Subcuticular tissues were closed with 2-0 Vicryl, and the skin was closed using staples.
Sterile dressing was applied over the wound. The patient was then transferred to the postoperative care unit in stable condition.


Postoperative X-ray showing AP and lateral views of the right knee
The recovery of the patient was unremarkable. She was able to walk the same day of the surgery. The pain was well managed with oxycodone and acetaminophen. Aspirin was used for DVT prophylaxis. The sutures were removed uneventfully.
The initial active range of motion was from 5 to 90 degrees which gradually increased to 3 to 120 degrees after a month of physical therapy. She demonstrated a full range of motion without any pain at her 3 months follow up visit. The patient was now back in her routine. She was happily doing yoga and enjoyed fencing as she did before the onset of pain.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 14, 2025.
