An 81-year-old female presented to our office with complaints of worsening pain in both knees (left greater than right). She stated she sustained a work-related injury 14 years ago injuring both her knees and shoulders.
She worked as a registered nurse, currently not working. She was presently staying with her granddaughter and loved to move around and cook. Over the past year, she had increasing pain and stiffness in her left knee. She was unable to perform her daily activities. Activities such as walking up and down the stairs, bending, and sitting for prolonged time exacerbated her knee pain.
Previously, she has had knee interventions in the form of cortisone injections and hyaline injections. She also tried other conservative management options in the form of physical therapy and heat pads. She stated she had minimal relief which didn’t last with conservative management.
The patient had comorbidities in form of diabetes mellitus which was well controlled with oral hypoglycemic agents. She stated her most recent HbA1C was 6.0 signifying good control. Her past surgical history included anterior cervical decompression with fusion done 2 years ago. She had no known drug allergies.
She described her pain as a dull ache which was moderate in intensity. The pain was located diffusely around the knee but was greater on the inner side of the knee. She reported joint crepitus as an audible sound created by bones rubbing against each other. She denied any instability or laxity about the knee and denied any twisting injury to the knee.
Her physical examination revealed a steady gait with mild genu varus deformity. There was tenderness along the medial and lateral joint line and patellar facets. There was no evidence of clinical effusion. There were no skin scar or sinuses and mass/induration.
The range of motion of the left knee was full, with painful end flexion. Coronal, sagittal and rotational stress tests for instability were negative. There was no distal neurological deficit. Bilateral lower extremity pulses were 2+ and comparable. Examination of the right knee, bilateral hip, and bilateral ankles were normal. Imaging studies revealed the presence of bilateral tricompartmental osteoarthritis.
After careful consideration of patient age, comorbidities, and lifestyle limiting knee pain, she was advised to undergo a custom left total knee replacement. Risks, benefits, and alternatives including nonoperative and operative management were discussed at length with the patient. She agreed to undergo left custom total knee replacement.
A preoperative CT scan of the patient’s left knee with the hip and ankle was obtained a few weeks before the procedure. The CT scan data was used to construct a unique patient-specific implant considering the patient’s unique anatomy. Disposable 3D constructed instruments and jigs were obtained after processing of patients’ data. A preoperative plan was formed to aid in the correct alignment of the artificial knee joint. These tools ensured the surgeon was equipped for a successful surgery replicating the natural knee.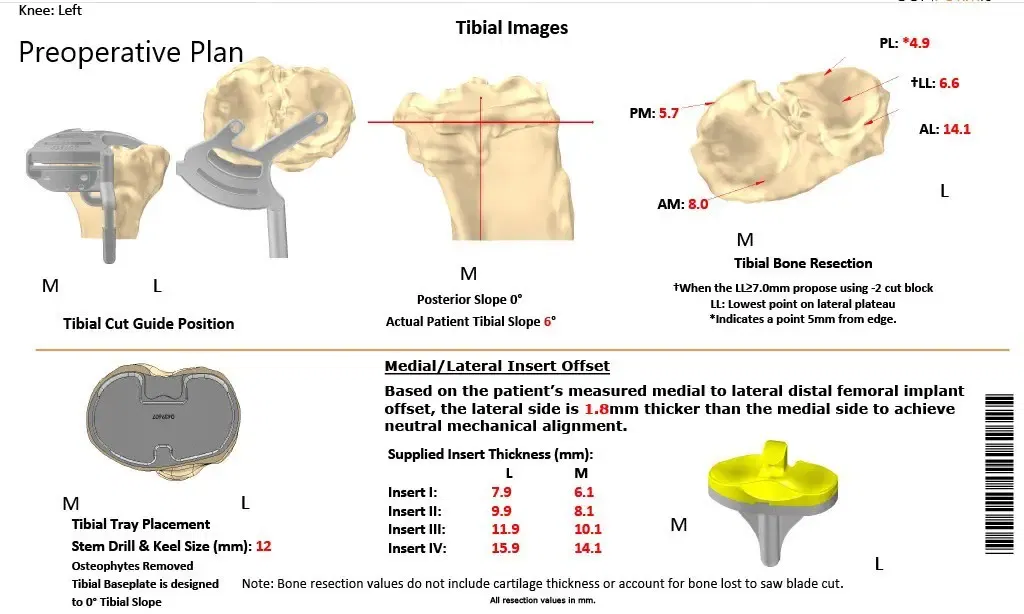
Complete Orthopedics patient-specific surgical plan for a customized left knee replacement in an 81-year-old patient.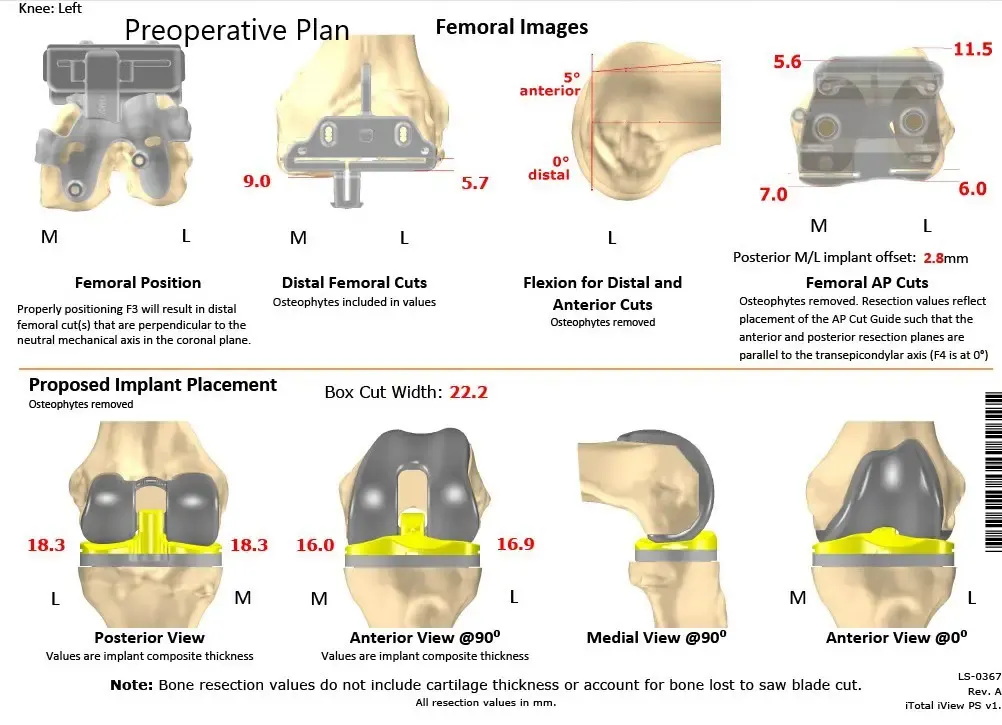
Complete Orthopedics patient-specific surgical plan for a customized left knee replacement in an 81-year-old patient (scan 2)


Preoperative X-ray images showing AP and lateral images of the left knee revealing tricompartmental osteoarthritis and severe medial joint space reduction.
The implant used: Custom femoral implant with a custom tibial tray, with 8-mm polyethylene insert, with custom 35-mm x 7-m patellar implant.
Description of the procedure: The patient Jas brought to the operating room after obtaining informed consent and signing the correct surgical site. The risks, benefits, and alternatives were extensively discussed with the patient prior to the procedure. The patient understands the increased risk of complications following the procedure.
The patient was then definitively positioned and the left lower extremity was then draped and prepped in the usual sterile manner. A straight incision was used for the arthrotomy. The skin and subcutaneous tissues were incised. Medial parapatellar arthrotomy was performed.
The tibia was then exposed. The tibial resection was then performed using the custom tibial guide. Attention was then turned tow rds the femur. The femur was then prepared using the customized guides. The distal chamfer and notch cuts were then performed. The tibial preparation was then performed, gap balancing was performed, and the gap was found to be correct.
Attention was then turned towards the patella. The patellar resection was performed. Drill holes were made in the patella and trial patella as then placed into position. The trial femur was placed into position, the trial tibia was placed into position, trial poly was placed into position. The knee was then reduced.
The knee was then trialed through a full range of motion. There was no flexion contracture. Full flexion was obtained. The patella tracking was excellent. The trial implants were then removed. The injection was given for postoperative pain relief. A thorough lavage was given. The bone was dried. The femur was then cemented into position.
Excess cement was removed. The tibia was cemented into position. Excess cement was removed. The poly was placed into position. The patella was then held in full extension with a bump under the ankle. The patella was then cemented into position. Excesscement was removed. The patella was held in position with the patellar clamp. After the cement hardened, thorough irrigation was given.
The medial parapatellar arthrotomy was closed with no 1 Vicryl and barbed suture. Cutaneous tissues were closed with O Vicryl. Subcuticular tissues were closed with 2-0 Vicryl. The skin was closed using staples. Sterile dressing was applied to the wound, and the patient was then transferred to the postoperative care unit in stable condition.


Postoperative X-ray images of the left knee in AP and lateral view.
Her recovery postoperatively was unremarkable. She maintained excellent control of her blood sugar levels with repaglinide 1mg BID and her pain was well managed with medications.
The surgical wound healed without any complications. She was able to walk with support the same day of the surgery. She continued physical therapy for muscle strengthening and increasing flexibility. Her home exercise program was continued. She reported excellent recovery in her follow-up visits. She was able to drive and move about the kitchen without the apprehension of pain.
She reported decreased pain on the right knee secondary to the offloading of the knee. The patient was extremely happy with her procedure she stated her knee felt natural. She would return for custom replacement of the right knee if needed.