When knee osteoarthritis no longer responds to non-surgical care, there are two main surgical paths. A high tibial osteotomy (HTO) realigns the shin bone to shift weight off the worn side of your own knee.
A total knee replacement (TKR) resurfaces the joint with metal and plastic parts. This page explains both, who each one suits, and how they compare.
About knee arthritis and malalignment
The knee is a hinge joint formed by the thigh bone (femur), shin bone (tibia), and kneecap. Smooth cartilage caps the bone ends, the meniscus acts as a shock absorber, ligaments keep the joint stable, a lining called the synovium makes lubricating fluid, and muscles bend and straighten the knee. When the bones line up correctly, your weight is shared evenly across the joint.
In osteoarthritis, these tissues gradually wear down, the cartilage and meniscus tear, and the joint becomes inflamed and stiff. If the leg is bowed (bowlegs) or knock-kneed, more of your weight passes through one side of the knee, wearing that side out faster. Age, extra weight, and past injuries all speed this up. Because cartilage and meniscus have little blood supply, they do not heal well once damaged.
Symptoms
Common signs of knee arthritis include:
- A grinding, popping, or clicking feeling in the knee.
- Trouble fully bending or straightening the knee.
- Knee pain, especially with activity.
- Stiffness after sitting or resting.
- Swelling around the joint.
How it is diagnosed
Diagnosis starts with your history and a physical exam, where the doctor checks for tenderness, swelling, warmth, range of motion, and how you walk.
X-rays show cartilage loss, bone spurs, and the alignment of the leg. An MRI or CT scan may be added if more detail is needed.
Blood tests can help rule out other causes such as rheumatoid arthritis, and in some cases fluid is drawn from the joint to check for infection or gout.

X-ray showing the knee joint and arthritis
When surgery is considered
Non-surgical care comes first: anti-inflammatory medicine, physical therapy, weight management, bracing, and injections such as cortisone or hyaluronic acid.
When arthritis is advanced and these non operative treatments stop helping, surgery becomes the conversation, and the two main options are a high tibial osteotomy and a total knee replacement. Which one fits depends mostly on your age, how much of the knee is worn, and your alignment.
High tibial osteotomy: who it suits
An HTO keeps your own knee, so it is aimed at people with earlier, one-sided arthritis. It tends to suit someone who is generally younger than 60, has wear limited to one side (compartment) of the knee, still bends and straightens the knee well, and has stable ligaments.
It is not suitable for people who are significantly overweight, have inflammatory arthritis like rheumatoid arthritis, or have arthritis behind the kneecap (patellofemoral arthritis).
Types of high tibial osteotomy
There are two main ways to realign the bone, and both are held in place while it heals, usually with a plate and screws (sometimes a cast):
- Lateral closing wedge: a measured wedge of bone is removed from the outer side of the upper shin bone to correct the angle.
- Medial opening wedge: a cut is made on the inner side of the upper shin bone, opened up to the right angle, and the gap is usually filled with a bone graft.
The high tibial osteotomy procedure and recovery
Osteotomy literally means cutting bone. The surgeon cuts and reshapes the upper shin bone near the knee to change its angle, moving your weight off the worn compartment and onto the healthier side. This relieves pressure and can slow the arthritis.
Recovery takes patience because the cut bone has to heal. Full weight on the leg is delayed, and you may use crutches for up to 12 weeks, with regular physical therapy to rebuild movement and strength.
Full recovery can take several weeks to months, and some people still have some residual pain afterward.
Risks of high tibial osteotomy
As with any bone surgery, there are risks to weigh:
- Infection or knee stiffness.
- Injury to the nerves that work the foot or the blood vessels supplying the leg.
- The bone failing to heal (non-union), which can need a second surgery, and possible problems at the bone-graft site.
- A small change in leg length, longer or shorter.
- Pain relief that is not always predictable.
- The chance that you still need a total knee replacement later, and that the replacement is more difficult after an HTO.
Total knee replacement
A total knee replacement resurfaces the worn joint with artificial parts. The end of the thigh bone is capped with a metal piece (the femoral component), the top of the shin bone gets a metal tray (the tibial component), and a durable plastic insert (cross-linked polyethylene) sits between them to glide like cartilage. The metal parts are usually fixed to the bone with bone cement.
In one common design (called posterior-stabilized), a small post on the plastic and a matching notch on the metal work together to do the job of a knee ligament, keeping the joint stable as it bends. The goal is to recreate the knee’s natural movement and alignment.
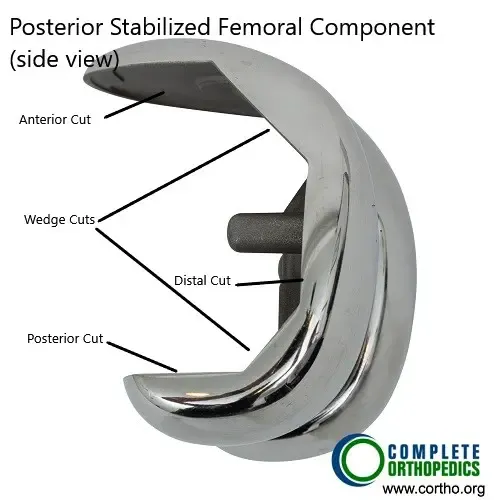
Femoral Component (side view)

Tibial component (undersurface)
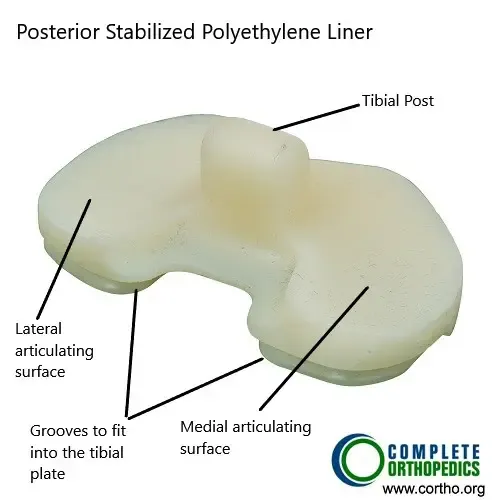
Polyethylene Insert (Posterior Stabilized)
Benefits and recovery of total knee replacement
Unlike an HTO, a knee replacement can be done at any age and works even when arthritis affects the whole knee rather than one side. Recovery tends to start sooner: most people bear weight the very next day and begin rehab early.
Modern implants commonly last well beyond a decade, pain relief is reliable, and satisfaction is high, with most people going about daily life without thinking about the knee.
If a replacement ever wears out, it can be revised. For these reasons, many surgeons now consider a knee replacement the better option for a lot of patients, even in earlier arthritis, when it is the right fit.
High tibial osteotomy vs total knee replacement
Both operations treat the same problem in different ways, and there is no single right answer. An HTO preserves your own knee and is appealing for younger, active people with arthritis in just one compartment, but it has a longer recovery, sometimes unpredictable pain relief, and often leads to a replacement down the road.
A knee replacement suits more widespread arthritis and older patients, offers faster early rehab and reliable pain relief, but it is a bigger commitment to an artificial joint. The right choice depends on your age, how much of the knee is worn, your alignment, and your goals, and it is a decision to make together with your surgeon.
Long-term outlook
A well-aligned HTO can slow or halt arthritis on the overloaded side and buy your natural knee more good years, though many people eventually move on to a replacement.
A total knee replacement tends to give complete, lasting pain relief, with implants that hold up well into their second decade. Your surgeon can help you weigh which path fits where you are now and where you want to be.
Insurance & Cost
High Tibial Osteotomy & TKR with Osteoarthritis of the Knee at Complete Orthopedics is covered by Medicare and most major insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), as well as most workers’ compensation and no-fault insurance plans. Your out-of-pocket cost depends on your specific plan, deductible, and the medical necessity criteria that apply to your case.
Call our billing team at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs. For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
Do you have more questions?
Can high tibial osteotomy (HTO) be performed on both knees at the same time?
While it is technically possible to perform HTO on both knees simultaneously, it’s not commonly done due to the increased risks and challenges associated with recovery and rehabilitation.
How long do the results of a high tibial osteotomy (HTO) typically last?
The results of HTO can be long-lasting, especially when combined with appropriate lifestyle modifications and physical therapy. This can last 5-20 years. However, the progression of osteoarthritis may continue over time, eventually necessitating further interventions such as total knee replacement (TKR).
What types of exercises are typically recommended during the recovery period after high tibial osteotomy (HTO)?
During the recovery period after HTO, gentle range of motion exercises, strengthening exercises for the quadriceps and hamstrings, and low-impact activities like walking or stationary cycling are usually recommended. Physical therapy will provide specific exercises tailored to individual needs and stage of recovery.
Are there any dietary or nutritional recommendations that can help support recovery after high tibial osteotomy (HTO)?
While there are no specific dietary guidelines for recovery after HTO, maintaining a balanced diet rich in nutrients like protein, vitamins, and minerals can support healing and overall health.
Are there any dietary or nutritional recommendations that can help support recovery after high tibial osteotomy (HTO)?
While there are no specific dietary guidelines for recovery after HTO, maintaining a balanced diet rich in nutrients like protein, vitamins, and minerals can support healing and overall health. Adequate hydration is also important for tissue repair and recovery.
Can high tibial osteotomy (HTO) be repeated if the initial surgery does not provide sufficient relief?
In some cases, a revision HTO may be considered if the initial surgery does not achieve the desired outcomes. However, the success of revision HTO depends on various factors, including the cause of failure and the condition of the knee joint.
Will I need to wear a brace or use assistive devices after high tibial osteotomy (HTO)?
A brace or assistive devices such as crutches or a walker may be recommended temporarily after HTO to support the knee joint and aid in walking during the early stages of recovery. Your surgeon will provide guidance on when and how to use these devices.
How soon after high tibial osteotomy (HTO) can I return to work or normal activities?
Most patients can expect to return to sedentary or light-duty work within a 4-6 weeks to a couple of months after HTO, with gradual progression to more strenuous activities over time. Heavy manual labor may require 3-4 months of rehab.
How does high tibial osteotomy (HTO) compare to other surgical treatments for knee osteoarthritis, such as partial knee replacement?
High tibial osteotomy (HTO) and partial knee replacement are both surgical options for treating knee osteoarthritis, but they differ in their approach and indications. HTO is typically recommended for younger, active patients with localized osteoarthritis, while partial knee replacement may be considered for select patients with damage limited to one compartment of the knee joint.
Will I be able to participate in sports or high-impact activities after high tibial osteotomy (HTO)?
Many patients are able to return to sports and high-impact activities after HTO, it’s important to discuss your specific goals and expectations with your surgeon.
Can high tibial osteotomy (HTO) be performed arthroscopically?
Yes, high tibial osteotomy (HTO) can be performed using arthroscopic techniques in some cases. Arthroscopic HTO may offer advantages such as smaller incisions, less tissue trauma, and potentially faster recovery compared to traditional open surgery. However, not all patients are candidates for arthroscopic HTO, and the decision will depend on various factors including the surgeon’s expertise and the specific characteristics of the patient’s condition.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.

