A 38-year-old male presented to our office with complaints of bilateral hip pain (right greater than left) for the last 5 years. The patient had a history of steroid abuse for the past 20 years. He was a professional bodybuilder with a history of non prescribed steroid use since he was 17 years old. He injected himself with anabolic steroids to promote muscle growth.
The pain was noticed 10 years ago while lifting weights at the gym. The patient ignored the pain and did not seek any medical attention. The pain subsequently worsened with an episode of sharp pain in the right hip joint about two years ago. The patient again did not seek any medical attention.
The pain worsened in the right hip to the point he was no longer available to work out in the gym or walk a few blocks without support. He was using a cane as an assistive device. He complained to increased discomfort on activities such as climbing stairs, bending, squatting, kneeling, and getting up from a chair.
The pain was constant and disturbed his sleep at night. The relief from pain was only temporary from the use of over the counter analgesics. The pain was located in the bilateral groins. The pain was described as a dull to sharp ache greater on the right side. The pain was moderate to severe in intensity.
He was an occasional smoker and a social drinker. He had no known drug allergies. He had no relevant medical or surgical history. There was an absence of any relevant family history. He was currently taking Lipitor and Alendronate which were prescribed by an outside physician for avascular necrosis of the hips.
On physical examination, he walked with an antalgic gait with an increased stance phase on the right side. There was no evidence of scoliosis or exaggerated lordosis. The bilateral shoulders, iliac spines, and the patella were the same level.
The examination of both the hips demonstrated tenderness at the anterior joint line. There was no swelling in the groin and no evidence of inguinal lymphadenopathy. There was no broadening or thickening of the bilateral trochanters. There was mild bi-trochanteric tenderness and rotational movements were painful in the right hip.
The sectoral sign was positive as demonstrated by differential rotation on hip flexion. There were no fixed deformities in both hips. The right hip range of motion was – flexion 0 degrees to 110 degrees, extension 0 to 5 degrees, adduction 0 degrees to 40 degrees, abduction 0 degrees to 20 degrees, internal rotation 0 degrees to 5 degrees and external rotation 0 degrees to 30 degrees. The range of motion of the left hip was full and unrestricted.
The examination of the bilateral knees and ankles was normal. The power, bulk, and tone of the bilateral lower extremities were normal. There was no distal neurological deficit. The bilateral lower extremity pulses were palpable and comparable. The deep tendon reflexes of the bilateral lower extremity were present and comparable.
Imaging was acquired in the form of X-Rays which suggested the collapse of the femoral head on the right side. There was a loss of sphericity of the right hip with sclerosis and subchondral cysts. The left hip had an intact contour. MRI was advised of the pelvis with both hips.
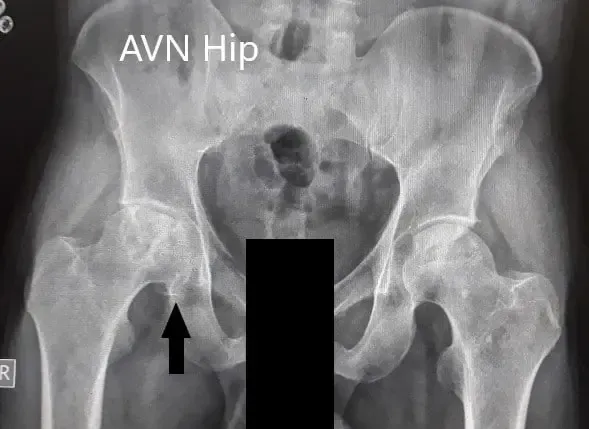
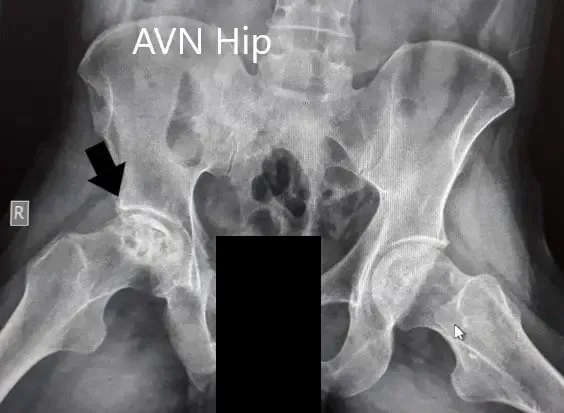
Preoperative X-Ray of the pelvis with both hips in anteroposterior and frog-legged lateral views
MRI suggested marked signal attenuation of bilateral femoral heads. There was a collapse of the right head and precollapse stage 2a of the left hip.

MRI showing bilateral femoral head AVN in T1WI

MRI showing bilateral femoral head AVN in T2WI


Axial sections of T1WI and T2WI showing bilateral AVN of the femoral heads
Based on MRI findings and physical examination, the patient has advised a right total hip replacement. The left hip demonstrated no collapse and the sphericity of the head was maintained. He was advised a core decompression surgery for the left hip.
Risks, benefits, and alternatives were discussed with patients at length. He agreed with the plan. The patient underwent a right total hip replacement. The left core decompression was guided towards the anterosuperior lesions. Bone marrow aspirate from the right iliac crest was harvested and then injected in the left hip.
