Partial and total knee replacement both treat the pain and disability of knee arthritis by replacing worn surfaces with metal and plastic parts. The difference is how much of the knee is replaced.
A partial replacement resurfaces just one worn section (compartment) of the knee, while a total replacement resurfaces all of it. A partial can feel more natural and recover faster, but a total knee replacement works for more situations and needs fewer revisions.
The right choice depends on your knee and specific situation.
About knee arthritis and the knee’s compartments
The knee has three sections, called compartments: the inner (medial), the outer (lateral), and the front, behind the knee cap (patellofemoral). Smooth cartilage covers the bones so they glide, while ligaments, the meniscus, and muscles keep the joint stable.
Osteoarthritis is the main reason for a knee replacement. The cartilage wears down over time, leading to pain, stiffness, swelling, and sometimes deformity. In some people the wear is limited to one compartment, which may suit a partial replacement. In others it affects the whole joint, which calls for a total replacement.
Symptoms
People with knee arthritis often have pain, stiffness, swelling, and trouble walking or climbing stairs. Pain tends to be worse with activity and better with rest. Some notice the leg changing shape (bowlegs or knock knees) or lose the ability to fully bend or straighten the knee.
How it is diagnosed
Diagnosis is based on your symptoms, a physical exam, and X-rays, which show the cartilage loss, bone damage, and any deformity.
Crucially, imaging shows whether the arthritis is in one compartment or the whole knee, which is what guides the choice between a partial and a total replacement.
Other problems can feel similar, including ligament injuries, meniscus tears, tendon irritation, bursitis, and inflammatory joint disease, so these are ruled out first.
When to consider knee replacement
Surgery comes after non-surgical care has been tried, including physical therapy, injections, braces, weight management, and pain medicines. A replacement is offered when those no longer control the pain and arthritis is limiting daily life.
Partial knee replacement
In a partial knee replacement, only one worn compartment is resurfaced. The surgeon works through a smaller incision, removes just the damaged bone surfaces, and leaves all the ligaments and other soft tissues intact.
A metal part is cemented onto each prepared bone end, with a high-grade plastic piece between them for smooth gliding, and most people walk the same day.
Not everyone is a candidate. A partial replacement is generally recommended only when:
- Only one compartment of the knee is affected.
- The knee is stable, with healthy ligaments (the ACL, PCL, and the collateral ligaments are intact).
- There is no history of meniscus surgery in another compartment.
- The person has a less demanding lifestyle.
- The person is not in the obese BMI range.
- There is no inflammatory arthritis such as rheumatoid or reactive arthritis.
- There is no significant deformity (bowlegs, knock knees, a knee that will not fully straighten, or one that cannot bend past 90 degrees).

X-ray showing a partial knee replacement of the patellofemoral portion of the knee joint
Total knee replacement
In a total knee replacement, the worn surfaces in all three compartments are resurfaced. The bone ends are shaped so the metal parts fit securely, with a plastic insert between them.
It is recommended when arthritis affects more than one compartment, or when there is deformity, ligament damage, or meniscus problems, because the surgery can also correct the alignment and rebalance the knee.
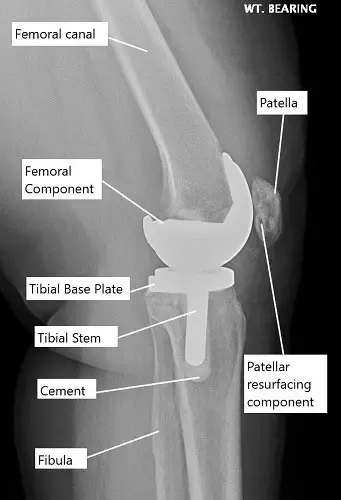
X-ray showing a total knee replacement.
Partial vs total: the trade-offs
A partial replacement has some clear short-term advantages. The surgery is shorter, and the risks that come with knee replacement (blood loss, nerve injury, blood clots, infection) are lower because less tissue and bone are disturbed.
Because the ligaments are kept, the knee tends to feel more natural. Part of that is proprioception, the position sense carried by nerves inside the ligaments that tells your brain where your limb is. A total replacement sacrifices some of those ligaments, which is why some people describe a total knee as feeling more mechanical. Recovery from a partial is usually quicker, with less pain.
Even so, a partial is done less often, for good reasons. Arthritis can later spread to the other compartments, so many partial replacements eventually need revision to a total, and that revision is more complex than a first-time total replacement.
A total also corrects deformity better, handles later ligament or meniscus damage, and is the right choice for inflammatory arthritis, which involves the whole joint. Because of the lower revision rates, many people who could have a partial choose a total.
Deciding between partial and total
The choice usually comes down to a few factors:
- Extent of arthritis: a total is needed if more than one compartment is affected.
- Age and activity level: younger, active people may value the natural feel of a partial, while older people with less demanding routines may do well with a total.
- Overall health: someone with other health issues might prefer a partial to shorten time under anesthesia and in the hospital.
Recovery
For both surgeries, most people walk the same day or the next day and start physical therapy early. Recovery tends to be quicker after a partial replacement because less bone and tissue are removed, though full recovery for either can take several months. Sticking with therapy and home exercises is what restores strength, motion, and balance.
Risks
Both carry the general risks of surgery, including infection, blood clots, bleeding, nerve injury, and stiffness. A partial replacement has lower risk overall because less tissue is cut.
Its main downside is that it may need revision later if arthritis spreads to the other compartments, and converting a partial to a total can be more complex than a first-time total replacement.
Long-term outlook
Both surgeries give strong long-term results, with major pain relief and better mobility for most people. A total replacement has lower revision rates and is preferred by most patients once they qualify. A partial feels more natural but may not last as long, because arthritis can still develop in the compartments that were left alone.
Protecting your knee long-term
Whichever surgery you have, low-impact activities like cycling, swimming, and walking help keep the knee strong. Keeping a healthy weight, avoiding twisting, heavy lifting, and high-impact sports, and treating new injuries early all protect the joint and help the replacement last.
When to see a doctor
See a knee specialist if pain, swelling, or stiffness limits daily activities, or if non-surgical care no longer helps. Seek emergency care if the knee becomes very swollen, hot, or red, or you cannot walk or straighten the leg, and after surgery, if you have fever, drainage, or sudden severe pain.
How Medicare Covers Total Knee Replacement Implants
If you have Medicare, your healthcare provider may bill for CPT Code 27447. This is a surgical procedure where the damaged knee joint is removed and replaced with an artificial knee.
If you have Medicare, your healthcare provider may bill for CPT Code 27446. This is a surgical procedure where only the damaged inner (medial) compartment of the knee is removed and replaced with an artificial implant, leaving the healthy parts of the knee intact.
What is the out-of-pocket cost:
Estimated Out-of-Pocket Cost for Total Knee Replacement Implants (27447): $259.73
Medicare approves about $1,298.63 for this procedure and pays 80% of it ($1,038.90). The remaining 20% is the patient’s responsibility.
“For example, hypothetical patient, Stacy, needed a total knee replacement. Her procedure was a replacement of her knee joint with an artificial implant (27447). Thanks to Medicare, her total out-of-pocket cost was about $259.73. Her secondary insurance then covered it completely!”
Estimated Out-of-Pocket Cost for Partial Knee Replacement Implants (27446): $232.94
Medicare approves about $1,164.69 for this procedure and pays 80% of it ($931.75). The remaining 20% is the patient’s responsibility.
“For example, hypothetical patient, Joan, had arthritis limited to the inner part of her knee. Instead of a total knee replacement, her surgeon replaced just the medial compartment with an artificial implant (27446). Thanks to Medicare, her total out-of-pocket cost was about $232.94. Her secondary insurance then covered it completely!”
For insurance and cost information, see our Insurance Information page.
Do you have more questions?
Are there any age restrictions for either PKR or TKR?
There are no age restrictions for either procedure. The decision is more dependent on the patient’s overall health, activity level, and the extent of joint damage rather than age alone.
How long do the implants from a PKR and TKR last?
Partial Knee replacement implants can last 10-20 years or more, but total knee replacements typically have survival greater than 20 years.
What is the risk of infection with knee replacement surgery?
The risk of infection is low, typically around <1% for knee replacements.
Can I undergo a PKR if I have had previous knee surgeries?
Yes, you can still be a candidate for PKR after previous knee surgeries, depending on the condition of your knee and the type of surgeries performed. Each case needs to be evaluated individually.
What is the success rate of PKR and TKR?
Both surgeries have high success rates, with many patients experiencing significant pain relief and improved mobility. Success rates can exceed 90% depending on the circumstances and the surgeon’s expertise.
Can I play sports after knee replacement?
While high-impact sports are generally not recommended after knee replacement, many patients can return to low-impact activities like swimming, cycling, and golf.
What is the risk of dislocation with PKR and TKR?
The risk of dislocation is more relevant to hip replacement. For knee replacements, the concern is not dislocation but rather implant loosening or wear over time.
How do I prepare for knee replacement surgery?
Preparation typically involves several preoperative tests, discussions about anesthesia, and possibly banking your own blood for transfusion if needed. It also involves planning for postoperative care and rehabilitation.
How long will I stay in the hospital after surgery?
The stay can vary; PKR patients may go home the same day or after one night, while TKR tend to stay 1 day. Healthier patients can go home the same day.
How do I care for my knee after surgery?
Post-surgery knee care involves managing pain, preventing infection, attending physical therapy, and gradually increasing activity levels under the guidance of your healthcare provider.
Can a PKR be converted to a TKR if needed in the future?
Yes, if arthritis develops in the other compartments of the knee, a PKR can be converted to a TKR. This is a common scenario and can be effectively managed with surgery.
What are the latest advancements in knee replacement surgery?
Recent advancements include the use of robotic-assisted surgery for greater precision, improvements in implant materials for increased longevity, and less invasive surgical techniques that aid in faster recovery.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.

