A total knee replacement usually relieves pain and restores function, but a small number of people find their new knee feels unstable and gives way. This is called buckling. It can make walking harder, raise the fear of falling, and chip away at confidence. The good news is that buckling has identifiable causes and can usually be improved, often with physical therapy and sometimes with further surgery.
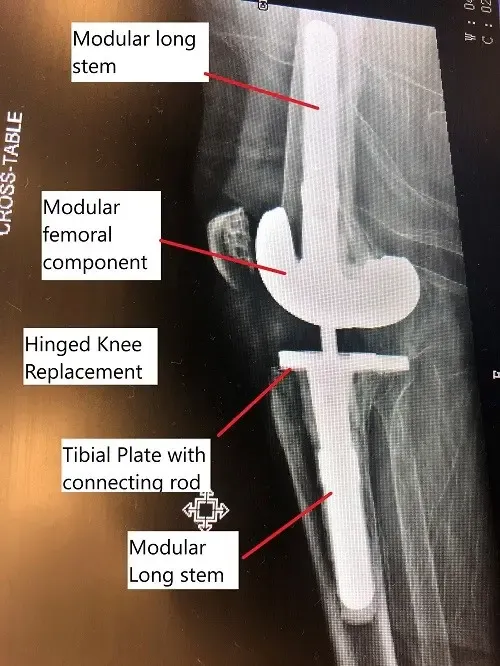
Xray image showing modular revision knee replacement.
What buckling after knee replacement is
Picture walking along and your knee suddenly gives out, so you stumble or nearly fall. That is buckling. After a knee replacement, it means a sudden, unexpected loss of stability in the knee, a feeling that it is giving way or cannot be trusted to hold your weight.
Why buckling happens
Buckling comes down to instability in the knee, which can have several causes:
- Weak muscles. Surgery disturbs the muscles and tissues around the knee, which can leave them weaker and less coordinated for a while.
- Loss of position sense (proprioception). Your body senses where your joints are. Changes in the joint and nerves after surgery can blunt that sense, so the knee feels unsteady.
- Surgical factors. Alignment that is slightly off, an implant that is not ideally positioned, or too much tissue release can leave the joint loose.
- Infection, implant loosening, or a poorly positioned implant, all of which can affect stability.
- Pre-existing deformities such as bowlegs or knock knees, which put uneven strain on the knee.
Who is more likely to get it
Buckling happens in only a minority of patients. It is more common in people who carry extra weight, have weak muscles, started with a deformity like bowlegs or knock knees, or are having revision (redo) knee surgery. People with rheumatoid arthritis or connective tissue conditions can also be at higher risk.
Symptoms of knee buckling
The main symptom is the knee giving way, but it often comes with others:
- A sense of the knee buckling, giving way, or feeling weak while walking or standing.
- Pain or discomfort in the knee, often around the episodes of instability.
- Swelling, which can make the knee feel even less stable.
- Trouble with weight-bearing tasks like climbing stairs or walking longer distances.
How buckling is diagnosed
Diagnosis starts with your history and a hands-on exam, where the surgeon checks the knee’s strength, alignment, and any obvious looseness.
Imaging such as X-rays, CT scans, or MRI is then used to check how the implant is aligned, look for loosening, and spot any bone or soft-tissue problems.
Types of knee instability
Surgeons describe a few different patterns of instability, which helps point to the cause and the fix:
- Side-to-side instability: the knee wobbles sideways, often when a deformity was not fully corrected or too much bone was removed.
- Bent-knee (flexion) instability: looseness front-to-back when the knee is bent, usually from implant sizing or angle.
- Mid-bend instability: looseness between about 45 and 90 degrees of bend, often from implant rotation or position.
- Backward over-bending (genu recurvatum): the knee hyperextends, sometimes from tightness in the band of tissue along the outside of the thigh.
- Global instability: a mix of the above, usually after major bone loss or several previous surgeries.
Conditions that can feel similar
A few other problems can mimic buckling, which is why an exam and imaging matter. These include the implant loosening, a meniscal tear, injury to other knee ligaments such as the ACL, and arthritis that was not fully addressed by the replacement.
Treatment options
Most people start with non-surgical care. Physical therapy is the cornerstone, with strengthening for the muscles around the knee (especially the quadriceps) to improve stability and reduce episodes of giving way.
A knee brace can add support and help alignment during weight-bearing, and anti-inflammatory medicines (NSAIDs) can ease pain and swelling, though they do not fix the instability itself.
If conservative care does not work, surgery may be needed. Options include revision surgery to replace or adjust the implant (sometimes using a more constrained design, such as a hinged or rotating-platform implant), repair or tightening of the ligaments and tendons when loose soft tissue is the problem, and realignment of the knee or implant to correct the instability.
Recovery after treatment
Recovery, especially after revision surgery, follows a structured rehab program with strengthening, gait (walking) training, and range-of-motion work. Full recovery can take several months, and you build back activity gradually with guidance from your care team.
Risks of treatment
As with any surgery, treatment carries some risk, particularly for revision procedures. The main ones are infection, blood clots in the leg (deep vein thrombosis), nerve injury around the knee, and the chance that the new implant loosens or fails again.
Preventing buckling after knee replacement
You cannot prevent every case, but you can lower the risk. Stick with your rehab program, avoid returning to high-impact activity too soon, and keep to low-impact exercise. Maintaining a healthy weight takes strain off the knee, and a diet with enough calcium and vitamin D supports the bone the implant relies on.
When to see a doctor
See your surgeon if your knee feels unstable, buckles, or hurts after a knee replacement. Seek emergency care if you have severe pain or swelling, signs of infection such as redness, warmth, or fever, or if you fall because the knee gave way.
For insurance and cost information, see our Insurance Information page.
Do you have more questions?
What are the potential complications of revision TKR surgery for buckling?
Complications of revision TKR surgery for buckling may include infection, implant failure, persistent instability, stiffness, or nerve damage. However, these risks can be minimized with careful surgical planning and post-operative management.
Is there a risk of recurrence of buckling after successful treatment?
While recurrence of buckling after successful treatment is possible, it’s less common with appropriate rehabilitation and adherence to preventive measures. Close follow-up with healthcare providers can help monitor for any signs of recurrence and intervene as needed.
Are there any alternative treatments for buckling after total knee replacement?
In some cases, alternative treatments such as regenerative therapies or adjunctive procedures like nerve blocks may be considered for individuals who are not candidates for or prefer to avoid surgical intervention. However, the effectiveness of these treatments may vary, and consultation with a healthcare provider is recommended.
How can I manage fear of falling after experiencing buckling episodes?
Managing fear of falling after experiencing buckling episodes involves a combination of physical therapy to improve strength and balance, psychological support to address anxiety and apprehension, and environmental modifications to reduce fall risks at home and in the community.
Can buckling after total knee replacement affect my ability to return to work or participate in recreational activities?
Yes, buckling after total knee replacement can impact your ability to perform daily activities, work tasks, and recreational pursuits. However, with appropriate treatment and rehabilitation, many individuals can regain confidence and resume their desired level of activity.
Are there any long-term consequences of experiencing buckling after total knee replacement?
Long-term consequences of experiencing buckling after total knee replacement may include continued instability, joint damage, and reduced quality of life. However, early detection and intervention can help minimize these risks and improve outcomes.
How can I find a healthcare provider experienced in treating buckling after total knee replacement?
Finding a healthcare provider experienced in treating buckling after total knee replacement involves asking for referrals from your primary care physician, researching specialists in orthopedic surgery or sports medicine, and seeking recommendations from other patients who have undergone similar treatment.
Is there ongoing research into better treatments for buckling after total knee replacement?
Yes, ongoing research aims to identify better treatments for buckling after total knee replacement, including advances in surgical techniques, implant design, rehabilitation protocols, and adjunctive therapies. Participating in clinical trials or studies may offer opportunities to access innovative treatments and contribute to scientific knowledge in this field.
Can buckling after total knee replacement affect my overall quality of life?
Yes, buckling after total knee replacement can significantly impact your overall quality of life by limiting mobility, causing pain and discomfort, and affecting your ability to perform daily activities and participate in social or recreational pursuits. However, with appropriate treatment and support, many individuals can experience improvements in symptoms and regain function.
Are there any lifestyle modifications I can make to help manage buckling after total knee replacement?
Yes, lifestyle modifications such as maintaining a healthy weight, avoiding high-impact activities, using assistive devices as needed, and practicing fall prevention strategies can help manage buckling after total knee replacement and reduce the risk of further injury.
Can buckling after total knee replacement be a sign of implant failure?
Yes, buckling after total knee replacement can be a sign of implant failure, particularly if it occurs suddenly or is accompanied by other symptoms such as pain, swelling, or decreased range of motion. Prompt evaluation by a healthcare provider is important to identify and address any underlying issues.
How can I stay active and maintain fitness after experiencing buckling after total knee replacement?
Staying active and maintaining fitness after experiencing buckling after total knee replacement involves working closely with your healthcare team to develop a personalized exercise program that addresses your specific needs and limitations. This may include low-impact activities such as swimming, cycling, or strength training, as well as modifications to accommodate any residual symptoms or functional deficits.
Is there a support group or community for individuals who have experienced buckling after total knee replacement?
Yes, there are support groups and online communities where individuals who have experienced buckling after total knee replacement can connect with others facing similar challenges, share experiences, and provide mutual support and encouragement. These resources can be valuable for coping with the emotional and practical aspects of living with buckling and navigating the healthcare system.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on June 30, 2026.

