The patient is a 37-year-old male who has been following up in our office for a complaint of right knee pain for the past year. The pain started a year ago and had an insidious onset. The pain is located in front of the knee and gets worse with activity, stairs and on trying to get up from a seated position. The pain is not associated with any numbness or tingling sensation.
The patient described the pain as moderate to severe in intensity and dull in character. The pain is constant and is not associated with any disturbance of sleep, weakness, or swelling. Activities such as walking, twisting, climbing stairs, and running make the symptoms worse.
The patient has been doing physical therapy for the past year with no relief. Medication such as ibuprofen makes his symptoms better only temporarily. The patient’s medical history is unremarkable and he had lower back surgery five years back following a motor vehicle accident.
The patient denies the use of any illicit drugs. The patient is a nonsmoker and does not take any medication currently. The patient denies any known drug allergies.

MRI of the right knee in axial section.
On physical examination, there was tenderness to palpation on the lateral wall trochlear groove, and the lateral patellar facet. The active range of motion was limited with flexion (130 deg), extension (5 deg.), and pain at extreme limits of the range.
The MRI of the right knee suggested patellar mal-tracking. Due to the failure of the conservative management, the patient was advised surgical management. The risks, benefits, and potential complications were all discussed at length with the patient. The patient agreed to go ahead with the procedure.
PREOPERATIVE DIAGNOSIS: Right knee patellofemoral pain.
POSTOPERATIVE DIAGNOSIS: Right knee patellofemoral pain.
OPERATION: Right knee arthroscopic lateral release.
DESCRIPTION OF PROCEDURE: The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. The right lower extremity was prepped and draped aseptically in the usual fashion. A tourniquet was applied and inflated during the surgery. The left lower extremity was put on a well-padded pillow. A time-out was called. The preoperative antibiotic was given. The arthroscope was set up.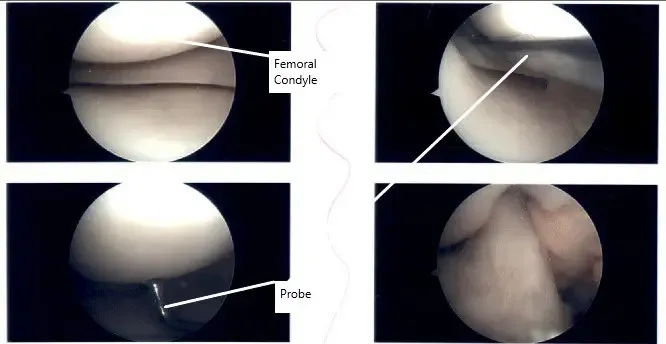
Intraoperative right knee arthroscopic images
A lateral entry portal was made and the arthroscope was introduced. Medial entry portal was made. Examination of the meniscus and ACL showed that they were intact. Patellar maltracking was checked and found that the patella was laterally set in the initial 30-degrees of motion. On deep flexion, the patella was well set in the trochlear groove.
A decision of lateral release was made. The scope was entered on the medial side. A blunt trocar was entered and a tunnel was made lateral to the lateral capsule. The ablator was introduced and lateral release was performed. Using the ablation, hemostasis was achieved by coagulation of vessels.
The tourniquet was released and the saline supply was stopped to find out any bleeders and hemostasis was achieved thoroughly. The knee was irrigated and drained. The closure was done using #3-0 nylon. Marcaine 10 ml was Depo-Medrol were injected into the knee.
The dressing was performed using 4×4, Webril, and Ace wrap. The knee immobilizer was applied. The patient was extubated and moved to recovery in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 8, 2025.
